SURVIVAL FACTOR IN NEOPLASTIC AND VIRAL DISEASES
By
WILLIAM FREDERICK KOCH, Ph.D., M.D.
Chapter 15
TERMINATION OF THE MALIGNANT PHASE RESTORATION OF THE FUNCTIONAL CARBONYL GROUP
We have already explained the two activated Carbonyl groups of our Postulate: One that initiates the oxidation progression and transfers the energy produced to carrier phosphate bonds. The other receives the energy from these bonds, and passes it on to the working mechanism of the cell, the contractile, the conductile, the secreting, or the mitotic fibrilla and units. They can both be blocked in their functions, by inactivation of their activating ethylenic linkages, or by a firm condensation with an amine group of some pathogen. When this takes place energy does not pass to the functional unit by the normal controlled route and only fermentation or Krebs Cycle energy is produced to pass directly into the working unit. Thus excessive contraction as the spasms of bronchial asthma, or excessive secretion as the secretion of hay fever, or excessive synapse closure as in some phase of insanity, a compulsion neurosis, etc., or impulse generation as of ticdoulereau, or excessive uncontrolled mitosis as of neoplasia will have to be the result in the tissue that is affected. The functional fault is demonstrated in the uncontrolled nature of the act, and all may be classified as allergies (Koch, Natural Immunity, 1934, and Cancer and Its Allied Diseases, 1929, where we attributed the abnormal energy transfer to a photosensitization process).
The correction is, of course, the restoration of the normal FCG activity in both capacities. That this can be accomplished no matter what the allergy happens to be is illustrated further in this section. Many more cases could be given in all categories, especially in the common allergies where the cure rate ran over 80% in the Court Testimony, but what is given is enough to illustrate.
The speed of the recovery is shown very well in the allergies of the respiratory system, and in the cure of the compulsion neurosis case, but it is also seen in the neoplastic category, too, as is illustrated immediately by biopsy tests or in the long run by the surgical tests outlined farther on. It is to be emphasized that the cure or correction of the disease in any instance is the restoration of the normal FCG function and the cleaning out of the debris and restoration of the normal structure and function, as the case requires. Then the normal being established, it can be broken down perhaps again when circumstances force this change. There may be some immunity or increased resistance due to a Carbonyl substitution for the ethylenic activation of the FCG, at any rate, though many cases stay well after being cured of cancer for several decades, there is no absolutely permanent and impregnable protection, and an understanding of the pathogenesis and what food diet means, is the best assurance of maintaining health after recovery.
There are some forms of primary cancer of the liver that are grossly pathognomonic. In such cases the expert surgeon can make a firm diagnosis without the biopsy, and he does so to protect his patient from embolism and hemorrhage incident thereto. This is not a matter of neglect, but of good judgment, and usually practiced. The type of greatest interest is that of diffuse distribution of myriads of small lesions over the surface and between the somewhat larger nodules that press up from underneath. The “feel” is also characteristic. In such cases there is deep jaundice because the smaller bile ducts are compressed or blocked by tumor tissue. The biopsy is characteristic also so that one can tell what the microscopic picture is from the gross features. In the diffuse type, the small surface nodules are much of the same size as if originating simultaneously, and thus speaking for a multiple origin of the carcinosis, a generalized equal distribution of the pathogen. As these nodules are smaller than many inside the liver, it is evident that the inner ones had an earlier start. Likewise, often, one lobe of the liver is more affected, especially the right lobe. Thus, in the beginning of the disease, the amount of pathogen is not so great that it makes an attack throughout all at one time. It is used up in one locality. However, at the terminal stage the myriads of small nodules equally and independently distributed speak for a swamping of the system with the carcinogen as if there were more toxins present than liver cells to combine with. Such a case will be described, and also a baby with a massive primary cancer of the liver proven by biopsy. This case is well described in the mother’s affidavit from which several points are reproduced. The series of photographs are also instructive. This information was sent us by Dr. M----, our collaborator, who had charge of the case, with his notes. The writer did not see this patient.
PRIMARY CANCER OF
THE LIVER
CASE No. 14
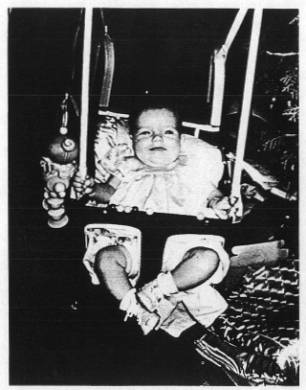
Judy McW., three months old. “After a normal birth, Judy, before the age of six weeks, showed signs of illness. Her abdomen was enlarged, she was restless, and her face did not show the repose of a healthy baby. Her physician could not find anything wrong with her until his check-up and examination at the end of her eighth week. At that time the doctor found her abdomen hard and much distended. During the period from August 20, 1948, to August 27, 1948, a tentative diagnosis of cancer was made and X-Rays were given although the X-Ray technician stated it was hopeless to expect a recovery.”
“By the time Judy was three months old the attending physician and another surgeon made an exploratory operation on Judy’s abdomen at which time a biopsy was taken. The physicians reported to us that the biopsy showed a high degree of malignancy, which involved 85% of the child’s liver. They told us that there was nothing that could be done to save Judy’s life; that we should take her home and make her as comfortable as possible for the few days she could live.”
“Her life expectancy was placed at 21 days. We were told not to remove the bandage from her abdomen lest the stitches burst out. It was the doctor’s opinion that the incision in her abdomen would not heal.”
“Dr. Koch’s Therapy was given by Dr. N. T. M., of Cisco, Texas. The dose was injected into Judy’s hip on September 18, 1948. At this time and during the course of Judy’s recovery, Mr. N took a series of color pictures showing her progress. Previously he had taken two pictures at six weeks of age and before the diagnosis of cancer. The series of pictures gives a good idea of her case.
“At the time the injection was given, Judy’s abdomen was so much enlarged that she could hardly breathe due to upward pressure on her lungs. The circulation on the surface had greatly increased and she had a bluish cast from a diffusion of blood in and just under the skin. Veins under the skin of the abdomen were plainly visible. The abdomen was very firm, even hard. At the time the Koch Treatment was given, Dr. M. expressed no hope of securing a recovery as he thought the case was too far advanced.
“Within ten days after the Treatment Judy showed definite reactions which raised our hopes. Shortly, she began to pass large quantities of mucous with bowel movements. She also passed a large amount of water in the normal manner, sometimes requiring as many as twenty diaper changes per day. No medication was used after the injection of the Koch Treatment, and only minor changes were made in the baby’s diet, Apple juice was substituted for orange juice, and Judy liked it. After Treatment was given and until recovery was practically complete, only one doctor saw Judy that was a doctor residing at Azle, Texas, who removed the stitches from the healed incision about the middle of October 1948.
“Soon Judy began to gain weight and her abdomen rapidly reduced in size and became more soft and pliant so that she could breathe better. The hard growth receded toward the lower right side. By December 25, 1948, she had a healthy and normal appearance as the pictures mentioned before show, but some traces of the growth remained.
“Later, about May 12, 1949, I had her examined by a doctor in Paris, Texas. He could find nothing, after which he was told of the baby’s former illness and he could still find no trouble.
“On November 11, 1949, Judy and her mother appeared before a group of physicians and surgeons especially interested in cancer who met at the Blackstone Hotel in Fort Worth, Texas. While before this group, more than one doctor examined Judy and nothing was found wrong with her.
“On February 18, 1950, both parents and Judy attended a meeting of physicians at Tampa, Florida. Here Judy was again shown to the group of doctors. These were most friendly to the Koch Treatment. Judy is now past two years old. She has shown a normal growth and development, normal mental development, and absolutely no abnormalities that we are aware of. She is very active, mischievous, and friendly. She has had practically no illness after taking the Koch Treatment and recovering from cancer.” These statements by Judy’s parents are signed and notarized.
Dr. M---- sent a more technical account, which adds nothing to the facts given by the mother. This mother’s report should be studied. The observations are well made, and any physician who is experienced, can get a great deal of information out of them. The steady progress of the pretreatment period is plainly established. The manner of absorption of the neoplasm shows it was not of the diffuse type as the next case demonstrates, but was a massive cancer starting in the right lobe of the liver, and of very high (grade IV) malignancy no doubt. The block in the portal circulation was not due to destruction of the vein, but to simple pressure, and the quick relief had, shows also in the better bowel and kidney action as the massive growth underwent absorption. This case should be compared with Case No. 15, “Diffuse Type Primary Cancer of the Liver.”

No. 1. Taken before the injection, September 18, 1948.

No. II. Taken at the time of the Treatment September 18, 1948.

No. III. Taken several weeks after Treatment.
No. IV. Taken a few weeks later.

No. V. Six months after Treatment.

No. VI. Taken a year later.

No. VII. Taken a few years later.

No. VIII. Taken September 1960, twelve years after Treatment.
DIFFUSE TYPE
PRIMARY CANCER OF THE LIVER
CASE No. 15
Prof. R. S. L.
Mr. Geraldo A., early in March 1941, showed loss of appetite, progressive loss in weight and weakness. Dr. O. A. L. examined him and found a large tumor in the abdomen. The patient was conveyed to Rio de Janeiro and placed in the hospital of the Beneficiencia Portuguese where he was operated by Professors R. L. and J. M. G. and helped by the assistant physician. Laparotomy disclosed an extensive neoplasm of the liver that had infiltrated the colon extensively. So extensive were the infiltrations and so widely had it spread, the operators decided it was impossible to give any surgical aid. Further, the type of liver cancer was so definite it was not necessary to remove a biopsy to add to the information already provided by the laparotomy findings.
The writer examined the patient together with his surgeons and Prof. R. S. L. seven days later. The patient could not turn in bed, was vomiting black bile or blood continuously, could not eat, and was of a dark jaundice color, very thin, in fact so emaciated that one could feel the diffuse nodules over the whole liver surface as it bulged forward and extended down into the pelvis. His doctors said he might live a week or two but certainly not longer.
We gave him an injection of a Parabenzoquinone solution, 2cc. containing two micrograms in solution, on July 15, 1941. The patient, who up to that time had been showing only a light fever, had a severe chill three days later, and a fever of 39°C. On July 25th, he belched much gas, and had intense gastric pain for only a short time. The tumor steadily absorbed, and concomitantly his weight and strength returned. The jaundice faded and he gained 20 pounds in weight, was able to walk, and returned to his home in Barbacena where his health gradually returned. On October 3rd, he had another reaction with a chill and fever of 39°C., and a general oedema was shown. Everything yielded spontaneously, and the patient gaining then over 40 pounds had completely recovered and was back to work. The report in April 1953, and again in 1955 shows he is still in excellent health and cured.
CANCER OF THE
STOMACH
CASE No. 16
Mr. Wesley R. had a past history of severe gastric ulcer from 35 years of age until he reached 50. When he was 69 he had a more serious stomach trouble — pain and vomiting, with rapid emaciation, and loss of strength. Pyloric obstruction became complete. Several physicians made examination and found a tumor at the pyloric region. Dr. Demling operated him on June 28, 1926. A gastroenterostomy was done and a part of the tumor removed. The pathological report follows:

It is evident from this pathological report that the whole neoplasm was not removed and this is confirmed by the early recurrence of obstruction by the neoplasm.
Improvement was noted for only a few weeks and then the trouble recurred with more pain than ever and constant vomiting, rapid emaciation and cachexia. Dr. Harrison brought him to me on August 20, 1926. My examination revealed a large fixed tumor mass filling the epigastrium and extending below the level of the umbilicus. It was fixed to the liver, and bulged outward so as to be plainly visible and caused practically complete obstruction of the gastric outlet. The supraclavicular space on the left side showed a fixed lymphatic tumor as large as a walnut. There was considerable hemolysis. One dose of the serial systems of Carbonyl groups was given and recovery set in so that its effects were observed in a few weeks. The obstruction soon disappeared and he regained about twenty pounds to reach his normal weight in five months. Examination after the twenty-fourth week revealed no tumefaction. Radiographs show no tumefaction, but a stomach about one-third normal size, motility good. Only at the third, twelfth and twenty-fourth week periods were there reactions of note. Fever, tenderness in the stomach, loss of appetite, and a general achiness lasted about three days and then a much more pronounced improvement set in after each reaction. This improvement continued until full recovery was established. He has not had any stomach trouble since and enjoys vigorous health, works every day and walks to town in all sorts of weather as well as he did at fifty years of age. We heard from him last when he was 92 years of age and in good health, 23 years after Treatment. Certainly the restoration of the Survival chemistry was satisfactory in this case.
CANCER OF THE
STOMACH
CASE No. 17
Dr. W. Mantor
This was a case of cancer of the stomach equally far advanced as the former. His trouble started as indigestion in 1940. Radiographs revealed no pathology then. It soon changed to a progressive stomach complaint with constant pain and frequent vomiting, rapid loss of strength, and a weight loss from 150 to 120 pounds in less than a year. Several well-reputed clinics were tried in this year but the disease progressed. Radiographs made May 12, 1941, at the Tyler Clinic at Omaha gave a firm diagnosis of cancer of the stomach. At least two-thirds of the stomach wall was involved as the plates show. Exploratory operation at the Mayo Clinic within a week revealed massive involvement of the stomach wall, the pancreas, the glands about the aorta, and the liver. The supraclavicular glands of the left side were also involved. They gave a diagnosis of far advanced cancer, primary in the stomach, entirely inoperable, and hopeless, and sent him home.


On June 16 he was carried into Dr. Mantor’s office for Treatment. Dr. Mantor’s description includes the following, “extreme exhaustion, anemia, hemolysis, cachexia. No crenation of red blood cells in a one percent NaCl solution (all should crenate). Linear scar from exploratory operation, massive induration of the epigastrium, readily palpable and bulging forward so one could see it easily as he lay down. Since one year previously an X-ray of the stomach showed no pathology whatsoever, this neoplasm was very malignant and rapidly progressive and destructive.”
One injection of 2 cc. of the 12X dilution of the serial system of Carbonyl groups was given June 16, 1941. In a few days he started to feel better and soon took up the farm he had to leave because of the sickness. Nine weeks after the Treatment, examination could reveal no tumor mass whatever. He had gained weight, color improved, and was more active. By the 12th week, he could walk down the street rapidly without losing his breath and reported he was eating well and was feeling fine. By that time he had been working on his farm. There was no more cachexia. Dr. Mantor gave him a second injection on September 8, 1941, during his 12th week. He continued towards complete recovery. A third injection was given two years later, September 1943.
Radiograph III, taken on June 14, 1944, shows his stomach after complete recovery. He was still well in 1947 when we last heard.

Radiograph I, Taken at the Tyler Clinic before treatment.

Radiograph II. Taken at the Tyler Clinic a few weeks after Treatment showing marked improvement.

Radiograph III. Taken June 14, 1944, after recovery. These radiographs are court exhibits.
The Survival Chemistry of course is concerned with the oxidation of burnable substances for energy production. Fuels and disease producing toxins, which come within its O/R potential ranges, are destroyed. The energy is used for doing work in the performance of function, and for the growth and repair. One can estimate the thoroughness with which the FCG system is restored by the rate of tissue reconstruction after the most devastating of cancers. The following two cases will illustrate.
METASTATIC CANCER
OF THE BOWEL
CASE No. 18
Dr. F. Richards
Mr. J. K. was 42 years old when X-Ray studies and exploratory operation showed widely metastasizing cancer of the splenic flexure of the colon, which caused complete obstruction. A colostomy was made at the Henry Ford Hospital at Detroit. The neoplasm spread rapidly throughout the abdomen and perforated the abdominal wall in several places as cauliflower growths with central fistulous openings that discharged feces and foul necrotic material. His general health deteriorated rapidly under the toxic strain, and the neoplasms grew proportionately rapidly under the same impulse. He had been a strong muscular man of 180 pounds swinging a heavy hammer all day when he took sick, and after the surgical aid he lost to 135 pounds, and kept on losing. The necrotic tissue in the abdominal wall had such a terrible odor it was necessary to slice away the most gangrenous part, and cauterize the borders to block the bleeding. The cauliflower fistulae took on greater speed thereafter. He was sent home to die, his case being entirely hopeless. On the way home he was examined at our clinic. Dr. Richards gave him an injection of the SSR Reagent on April 3, 1942. At this time the cauliflower growths were from 4 to 8 centimeters in diameter and equally high. During the following three weeks he did not show much improvement. Then he took a heavy reaction with such great congestion of the exposed cancer masses that another injection had to be given. The second Treatment was given at the beginning of the fourth week. Thereafter the bleeding quickly stopped and his whole condition rapidly improved. The cauliflower masses melted away and the abdomen was healed without leaving a visible scar. Palpation could reveal no more tumor masses after four more months. His bowels started to move normally through the rectum, and the colostomy stopped functioning. He gained weight to 113 pounds in June, and to 180 pounds in September when we sent him back to the Ford Hospital for repair of the colostomy, after he had returned to work a few weeks earlier.

This X-Ray was taken of Mr. J. K. on December 27, 1941 before Treatment.

His liver and other FCG’s that had been blocked by the carcinogen certainly went back to work for him, for he not only could digest food efficiently but was able to build up his tissue at the same time. His gain is shown in part in the Ford Hospital records as noted by Dr. Bohr. For the month of July, the record notes that he gained from 113 pounds at the first of the month to 175 pounds at the end of the month, that is a gain of 62 pounds in a month, or just two pounds or one kilo per day. This gain, we must add, was made on our vegetable, fruits and cereal diet, without any meat or animal proteins. The Ford Hospital documents, that were part of the Official Court Record, are worth studying. Some are appended. This gain in good solid flesh and blood on a vegetarian diet is not just an incident in this case. It is our experience, and meat eaters who cannot curb their appetites for animal food, should give these facts some consideration.
The following significant statements are taken from the Henry Ford Hospital record, the interval history taken by Dr. Bohr on August 28, 1942. “Patient left hospital April 1 of this year with a diagnosis of fungating Cancer of Colon and a terminal prognosis. On the way home that day, he received one of Dr. Koch’s ‘Cancer Cure Shots.’ . . . On July 1 he weighed 113 pounds, but from that time on he began feeling stronger and gained weight. By the middle of July, his wound was completely healed. His weight was 175 pounds at the end of July and he has maintained this weight ever since. He enters the hospital now, after being back to work for three weeks, for the first stage in a colostomy closure.”
This patient was examined at the Ford Hospital every year for many years and always found well. When last heard from he was still well. The radiographs show the obstruction of the bowel during the first weeks of his illness. The radiographs made after recovery are the same as any normal person’s. No adhesions or other sequelae are found, showing that the disease that existed formerly no longer exists.
What the Case Teaches:
Firstly, the Ford Hospital “General Memo” tells that they could not enter the abdomen to attempt a resection of the growth as it had infiltrated throughout and invaded the abdominal wall throughout. When one considers the position of the splenic flexure of the colon, back against the posterior abdominal wall and diaphragm, the distance to the umbilicus is twelve or more inches and as it had finally ruptured through the belly wall in three different places as large cauliflower fistulous growths, the amount of involvement was about total. It is important to realize this and also that the amount of infection, throughout the whole neoplastic involvement, was tremendous. Fecal fistulas always heal with a great amount of scarring and distortion and epidermal change consequent thereto. But in this case there was no scar left, nor epidermal change left to mark the areas of neoplastic or infectious involvement. The abdomen wall healed right through the skin without leaving a mark. The abdomen looked as clear as any normal baby’s that had never been sick. Just as the bowel function was restored so the colostomy became obsolete. So too, the only sequelae to the neoplasm were completely restored structure and function.
To the regular physician this fact is not comprehensible, and indeed if the other patients to be demonstrated here did not do likewise, one would scarcely have the courage to make this report. There is an explanation, however, and the case is offered with others as a demonstration of this explanatory observation. It is this. The recoveries in these cases after the SSR is used are different from those that take place under the flux of regular ordinary healing. This is due to the fact that after the SSR does its work no toxin, either carcinogenic or from a disease’s germs, is integrated with the protective fibrosis or the cancer cells. Before the SSR was used the toxin content was tremendous, if the odor, cachexia and rapid tissue destruction mean anything. The state of integration as we explain here, and in the Appendix, actually invited oxidative destruction of the toxins of all types, so that the fibrosis and cancer cells became obsolete and were absorbed by the ordinary autolytic procedures, so that nothing was left to interfere with normal tissue reconstruction. So normal reconstruction was not prevented and the normal rectifying tendency had full sway. It is such an observation, so often repeated, that makes one think that the normal state of man was such that he did, at one time in his perfect state, really possess an FCG of the order of the SSR or even more efficient.
SARCOMA OF THE
UTERUS
CASE No. 19
Mrs. McA., aged 43, was first seen on July 29, 1929. She was bedfast, emaciated, and exhausted. She had not rallied well from an abdominal exploration done by a very good surgeon two weeks previously to ascertain the cause of severe and frequent crises of vomiting and pain in the gall bladder region. The abdomen was found widely involved with neoplastic development from deep in the pelvis to the diaphragm, with the stomach, liver, and intervening structures heavily invaded. This was identified as the cause of the pain. A biopsy specimen was removed. The abdomen was closed as inoperable. The surgeon, Dr. Trimby, gave a biopsy report to us personally when he referred the patient. It showed a small round cell sarcoma of high-grade malignancy.
Our examination revealed a patient in bed, exhausted with weak pulse, sighing respiration, vascular shock, cyanosis, and an abdomen bulging with tumor masses, particularly on the lower left side. The liver and epigastric involvement could be readily palpated besides. The incision was not healed and appeared to be infiltrated with neoplastic extensions. This incision was made over the largest tumefaction within and it seemed that the neoplastic tissue underneath had invaded the abdominal wall. A photograph was taken and 2 micro micrograms of the Synthetic Survival Reagent were given.
She responded well up to the sixth week, gaining in strength and becoming rapidly free of the pain and vomiting attacks. However, at the beginning of the sixth week she started a reaction that continued to the middle of the ninth week.
It featured vomiting of a quite continuous nature whether she took food or not. No food was held. The pain feature that was so severe before Treatment was a minor matter, however. She lost weight and strength, and the dehydration was difficult to overcome. However, with the closing of the reaction at the middle of the ninth week she became very hungry and took on weight rapidly. For a few weeks she gained at the rate of five pounds a week, then at the rate of two pounds a week until she had reached 180 pounds. A slow gain followed to 200 pounds and then a slow loss to 180 pounds. Her health was fully established. All the tumefactions had disappeared before the end of the twelfth week after the Treatment. She is still in perfect health, according to our last report.

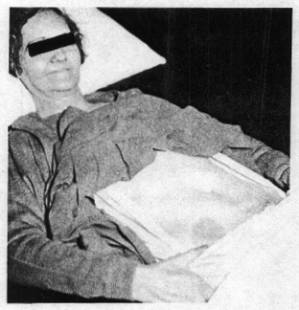
Photograph II, Taken after neoplasms were absorbed.
Another way to estimate the restoration of FCG activity is in the cure of Leukemia. Here in the terminal phases, the exhaustion of the blood forming organs can be so complete that leukopenia instead of the former leukocytosis is observed. The FCG’s required for cell construction are blocked, no doubt, by the carcinogen and both the red cell count and the white cell count are not able to be restored until the FCG’s are liberated and can go back to work again. The following cases are illustrative. Here the bad effects of irradiation are to be observed as well as those of the natural carcinogen. One might compare the response in a natural case of acute lymphatic leukemia with other cases that have been irradiated, or have reached the point of exhaustion and impending death. These latter states are about the same, showing how irradiation works on the blood forming organs. It kills them, as does the natural pathogen. Red and white blood cell restoration demonstrates FCG restoration.
ACUTE LYMPHATIC
LEUKEMIA IN A BOY
CASE No. 20
Dr. A. Guzman
P. F., age 12 years, treated January 8, 1956, by Dr. Guzman. His family history denied leukemia. The onset in the boy was rather rapid after a period of ill health. The symptoms were classical with petechial hemorrhages under the skin and in the mouth, cough, symptoms of anemia with great weakness. The red cell count was 1,500,000, the white were 232,000, lymphocytes in very great predominance, large mononoclonals and immature forms. The physical examination showed a blanched out boy with hemorrhagic spots of various sizes under the skin generally, especially the legs, arms and body. The gums bled, and the breath was foul. The mediastinal dullness was increased mostly to the right. The spleen and lymph glands were only moderately enlarged. He had a cough, was very weak and showed fever.
The injection of the Synthetic Survival Reagent was given, 2cc. of the 10-(12) solution. He was put on a supportive vegetarian diet. The recovery was steady with periodic reactions of chills and fever, general achiness, etc., as characterizes the recoveries under this Treatment.
The results showed in an improvement after each reaction until in August 1956, he was completely well. There were no signs of the disease left. The hemorrhagic spots had disappeared and the mouth was clear, the breath clean. The spleen and lymph glands were no longer enlarged. The spleen could not be palpated, and he was strong, had gained a normal weight and nutrition, etc. His platelets count was then 350,000, the red cells 5,100,000, white cells 7,200, polymorphs 76%. The coagulation time was normal. The only reaction of a focal nature was a sore throat, and that in a boy is difficult to interpret. However, it might mean that this was the site of the pathogenic toxin or virus production. This is especially suspicious, since the mediastinal glands were enlarged and the mediastinal dullness returned to normal with the recovery.
LYMPHATIC
LEUKEMIA WITH TERMINAL EXHAUSTION
CASE No. 21
Dr. Julian Baldor
Teddy S., age 14 years, in February, 1949, when treated by Dr. Baldor. He was referred by Dr. C with the report, “Chronic leukemia (proved by bone marrow biopsy) with hemorrhagic diathesis.” The exhaustion of the blood forming organs was seen in the fall in the blood count of whites to only 15,000, while the hemoglobin was 40% and the red cell count 2,150,000. His first diagnosis of leukemia was made six months previously from the high lymphocyte count, the hemorrhages under the skin and the gums, the weakness, enlarged spleen and lymph glands, the fever, pains in his legs and arms and the anemia. He was given 57 blood transfusions. These pepped him up a little at the start, but soon were found to be less effective and finally to be of no help at all. In fact, they were wasted on him. It was then he was sent to Dr. Baldor for the Koch Treatment.
Dr. Baldor’s examination showed an exhausted bleached-out boy, suffering with pain and fright, depressed, unable to walk, with an offensive odor from the mouth, profuse gingival bleeding, and generalized hemorrhagic spots under the skin. The mediastinal dullness was definitely enlarged and so also were the lymph glands generally increased with tubular breathing in the right lung base, and moist rales over the entire field. The liver and spleen were enlarged and tender. He was put on fruit juices and intestinal lavage for two days and then given 2 cc. of the SSR serial system of Carbonyl groups. The fever at the time was 102°F.
In a week he was sent home with a normal temperature. The spleen and liver were reduced in size, but not yet normal, the bloody patches had changed from a dark purple to a greenish color, and no new ones had formed. They then turned to yellow and finally disappeared. Nine weeks later he returned to Dr. Baldor for a check-up. He was able to walk and had gained 12 pounds in weight. The blood picture was red cells, 3,350,000, hemoglobin 52%, and leukocytes 8,000. At the twelfth week, he gave a reaction showing slight pains in the extremities for a few days, and a little epistaxis. The blood count then showed 4,000,000 red cells, white cells 6,500, hemoglobin 72%. He had gained 25 pounds in weight, felt perfectly normal in all respects: feeling, behavior, and in his physical findings.
It was reported to Dr. Baldor in 1957 that Teddy S. at the age of 21 was examined for military service and classified 1-A. This was seven years after being treated for what normally is a 100% fatal disease, in its terminal stage. Upon knowledge of his full previous medical history, he was re-classified. Dr. Baldor reported at that time that Teddy S. had held the best of health since his recovery, is married and is the father of a robust healthy child.
It is to be noted that after being seen by Dr. Baldor he did not receive even one blood transfusion, but gained in all respects on a vegetarian diet. It might appeal to one that the extreme exhaustion is not only a matter of lack of nutritional elements to support cell function, but even more a lack of energy to perform the functions of work and nutrition. The impediment to the mechanisms concerned blocked all activities including the burning of all sorts of toxins absorbed from the bowel, the mouth, tonsils, etc. Then, with the liberation of the tissue’s FCG systems, every impediment was burned out of the way and was kept out of the way thereafter.
MYELOGENOUS
LEUKEMIA WITH IRRADIATION LEUKOPENIA IN AN ADULT
CASE No. 22
Dr. Julian Baldor
Mrs. J. W. L., age 47 years, came on December 7th, 1948. She gives a history of an acute process with chills, fever, nausea and perspiration, six months previously following an influenza attack. Examination showed enlarged liver, enlarged spleen and enlarged cervical glands. The breath was offensive and the gums were bleeding. Some dental abscesses were present. Her blood picture showed red cells, 3,160,000, hemoglobin 57% and white count, 14,800, ploys, 88%, lymphocytes 10%, monocytes 2%. Both myelocytes and premyelocytes were present.
She had received two courses of X-Rays over the spleen and long bones, each of 600 R at an interval of 6 weeks. This did not improve her condition. The bleeding, weakness, fever and pains continued getting worse. Bone marrow slides showed definite abnormalities suggestive of Myelogenous Leukemia.
Because of the irradiation two doses of the SSR Reagent were given, one on December 13, 1948, and the other five days later. The improvement was prompt. The fever had left in five days. The enormous spleen that reached to the left iliac region, and the enlarged liver showed improvement and were less painful. The oral bleeding and infection likewise cleared up. The blood count March 15, 1949, showed red cells 3,850,000, hemoglobin 69% and leukocytes 8,500. Up to August 5, 1949, she gained ten pounds in weight. On June 16, 1949, the red cell count was 4,000,000, hemoglobin 72% and white cells 7,000. The chest signs improved slowly. By the end of 1950 her enormous spleen had receded to its normal position under the left ribs. The last blood count was taken May 1955 and showed red cells 4,150,000, hemoglobin 70% and leukocytes 3,500. She remains well.
This patient, like the others, was not given one blood transfusion after the SSR Treatment was started, and she improved on a strict vegetarian diet. Here the destructive effect of the X-Rays on the blood forming organs is easily seen, and the recovery of blood production could be better. The hemoglobin was only 70% when it should have been 80% or better and the white cell count could have been a thousand or two more. Thus the injury to the blood forming organs is not entirely corrected, and never will be, in line with our experience with the effects of irradiation. However, the gains made under this handicap when the FCG function is restored are well shown in this series of cases.
One should contrast these cases with the recovery from a slowly developing fatal form of bone sarcoma. Here it will appear that the rate of recovery is a function of the rate of development of the disease. It will be seen also that in the healing of the bone, the tissue is made much more dense and stronger than before the disease attacked it. Blood reconstruction is of this order, too.
ENDOTHELIAL
SARCOMA OF THE BONE
CASE No. 23
Mr. Harold B. was age 41 in September 1934, when he appeared for Treatment. He first noticed trouble with the right arm when he threw a ball some weeks previously. His family physician took some X-Rays and noted the sarcomatous status and sent him to the University of Michigan Hospital for thorough attention. The pain in the arm was sufficient to prevent its use, and motion was limited because of a hard swelling over the scapula. The X-Ray studies, blood studies and biopsies of soft and bone tissues led to the final diagnosis of Endothelial Cell Sarcoma of the bone. To reach this diagnosis, Paget’s disease, all other bone tumors were definitely eliminated. They gave him a hopeless prognosis since this type of sarcoma is always progressive and fatal, no matter how it is treated, but they offered to remove the whole shoulder girdle, if he wished. He refused and presented himself for our attention instead.

Our examination, made September 17, 1934, showed a lame right arm, a fist size mass over the spine of the scapula firmly fixed, and a walnut size mass closer to the dorsal spine and of the same texture as the other mass. Both were fixed to the underlying structures. There was some cachexia, but no tumor could be found in the abdomen or anywhere else. The X-Rays showed bone destruction extensively of the humerus and scapula, and neoplastic development between the two. The progress of the disease was slow and steady. The etiological factors as well as the tumor products were poisoning him, following a downgraded course.

The Synthetic Survival Reagent (SSR) was given in a dose of 2 cc. of the 10-(12) solution. There was no immediate sharp reaction, that is, in the next few days. The major reactions were at the 24th and 36th weeks. But he continued to improve slowly from the start. It took a few months to be able to use the arm without pain. In a year the tumors were completely absorbed, and an X-Ray showed nearly complete recovery in the bone, with considerably more denseness in bone structure. He was able to return to work and made a full recovery. Our next chance to make a radiograph was when he appeared in Detroit to testify for us in the Federal Court. The X-Ray made then showed full recovery and is reproduced here. He has remained well. Our last report was received in 1950. Ewing’s estimate of this disease is as follows, page 361, 1942 edition, Text Book on Cancer:
“Angioendothelioma, multiple endothelioma, diffuse endothelioma, or endothelial myeloma, the entire group, is characterized by predilection for the bone shaft, a tendency to multiplicity, a cellular and vascular structure, marked osteolytic properties, failure to produce tumor bone, and a relatively slow but fatal course.”
Radiograph I. showing condition before Treatment.


Radiograph II, showing condition after full recovery.
This relatively slow course as seen both in the progress of the disease, its cure and in the recovery process in the leukemia cases just given should be contrasted with the cases of J. K. and Mrs. MacA.
The University of Michigan records selected from the court records give the details sufficiently for a working idea. This record, like those of the other cases cited is voluminous. All other details are available to anyone who desires them. The radiographs should be studied also. The fact that the tumor is not confined to the bone but has grown between the bones and out over the shoulder shows it is not Paget’s disease. One should note this in the radiographs.
RECURRENT
METASTASIZED CANCER OF THE PALATE FOLLOWING SURGERY
CASE No. 24
Mr. A. J., age 60 years, was first seen by us on December 1, 1932. He gave a history of an attempt to remove one large and a few small growths from the hard and soft palates, by excision and touch-up cautery at the University of Michigan Hospital on October 15, 1931. The areas healed and all was well for a few months. Then the same type of growth reappeared over a wider area of the palate and enlargements formed in the neck and under the jaw. These were deeply fixed. The palate was well covered at the time of our examination. The large growth had returned with a dozen smaller ones around about it. The biopsy was squamous cell cancer.
We gave him the Survival Reagent injection and three days later he experienced a typical reaction. Generally a highly malignant cancer will give a recovery reaction twelve or twenty-four hours after the treatment is given and in the less malignant types as this one, the actions come as late as 72 or 84 hours after Treatment. But the symptoms are the same, namely a general achiness, chills and fever. All patients describe their reactions much alike, so we will give Mr. J’s description as an example. His Testimony stated, “About the third day I felt pretty badly. I became cold. I thought I was going to freeze. My wife put me in bed. We had the hot water bottles and about all the blankets we had to cover the bed with on me. It lasted possibly an hour. About three weeks from that time I had another cold spell, and for about six months, I believe, every three weeks, but they kept getting lighter.” The physical examination and careful questioning did not reveal any focus of infection, that contributed the toxin that excited the neoplastic change, as is so common in other cases. This case was probably a general viral infection.

After six months, no trace of any growth in the mouth, or in the neck, or under the jaw could be palpated. He remained well until a few years ago. It was reported he died of a stroke. He was then over 80 years old. There was no examination of the body to get the facts, however, only rumor.
In this case, as in so many that are biopsied or operated on, the recurrent growths are of a higher grade malignancy than when first touched with a knife, and that appears to be the case here, since the recurrence was rapid and the reactions so intense, though they came three days after the Treatment.
SARCOMA OF THE
SPLEEN
CASE No. 25
Dr. J. W. Kannel
B. G. was 6 years old when she was attacked with pain in the stomach and some fever. She had been experiencing an increasing difficulty in breathing for some weeks previously. Examination by Dr. J. W. Kannel revealed an enlarged spleen, enlarged axillary and inguinal lymph nodes, and a white cell count of 7,200. A few days later, June 23, 1943, the white cell count rose to 16,700, and on June 24th, it was 22,400. The aspect of the child was that of one very seriously sick. He immediately did an exploratory laparotomy, and found the spleen so greatly enlarged that it had compressed two-thirds of the left lung and had grown out against the intercostal muscles in ridges, so as to leave impressions of the ribs in between. The gross pathology was pathognomonic sarcoma of the spleen. It would have served as a good museum piece. It was besides, very hard and nodular, which is the case with spleen sarcoma. If it were an infection, it would have been soft and pliable. So the high white cell count was due to reticulo-endothelial disease, comparable to the high lymphocyte count in leukemia. Moreover, no abscess was found to account for the leukocytosis or the fever, which after all are characteristic of acute forms of cancer. Dr. Kannel did not do a biopsy, as he felt there was too much risk of causing uncontrollable hemorrhage or embolism because of the vascular structure of the organ, and because the gross findings were absolutely diagnostic without microscopic aid. Thus, his knowledge saved the patient from possible death resulting from embolism or hemorrhage.
On July 2, 1943, she was given 2 micro micrograms of the SSR and her recovery was gradual and steady until it was complete. The breathing became normal and so did the breath sounds. The projection of the spleen down into the abdomen 2 inches gradually subsided until it was of normal size. Her health became normal and so remains so far as we know. The last report was in 1956. One sees that the disease was corrected, and the straying tissues were normalized. The cause was removed right at its point of attack on the vital structure.
LYMPHOSARCOMA CASES
The call for lymphocytes to fight the toxins of chronic infection is standard experience. Though, the neoplastic hyperplasia no doubt had a protective purpose to start with (the reticulo-endothelial system always leads the combat against cancer) this type of hyperplasia does not accomplish any protection. It injures the patient just like the excessive production of poorly evolved thyroid secretion in Case No. I ., the toxic nodular goitre case. No doubt the interference with function was a matter of Carbonyl group block, as it was in the goitre cases, and so if this is true, the use of the Survival Synthetic Carbonyl Remedy should restore the normal functional efficiency of protection and the normal mitotic process. A few cases of different types of lymphocytic cell lymphosarcoma are given to illustrate the disappearance of neoplastic mitosis and the restoration of protection. This is seen in the return of the regular health and disappearance of the pre-growth signs and symptoms similarly in lymphosarcoma, as in the other forms of cancer.
It is the consensus, that lymphosarcoma is a generalized disease and indeed most cases, when seen first by us, showed generalized tumefaction of all palpable lymph nodes, increased dullness of the mediastinum, and great enlargement of the mesenteric glands. However, there is a type that grows up rapidly in one region without showing great involvement of other areas. This is the type that is most rapidly fatal and may indeed kill in a few months, after the onset. Such a case is the following:
LYMPHOSARCOMA
CASE No. 26
Dr. J. W. Kannel
Miss L. M., age 31, came under Dr. Kannel’s care in July 1925. Physical examination showed a tumor as large as a large orange involving the upper outer quadrant of the right breast and the axilla, which was completely and deeply involved. He removed most of the breast portion, but found the axillary development too deep to extirpate and left it in situs. The microscopic examination showed it to be a malignant lymphosarcoma. This tissue is not derived from the breast tissue itself, but seems to have its origin in lymphoid tissue. Characteristic of this type of lymphosarcoma, cachexia was developing rapidly, so Dr. Kannel prepared her for the Survival Reagent Treatment, and gave the injection on July 16, 1925. The presence of cachexia shows the extremely toxic status of the patient, both from the pathogenic toxin and from the products of the neoplasm intended to be protective, but which were toxic as the thyroid secretion in Case I.
Following the Reagent, there was rapid absorption of the axillary and other extensions of the neoplasm, with a simultaneously quick recovery from the cachectic state. She remained well until 1931, when a lump appeared in the left breast the size of one’s thumb. It grew rapidly also, as a heavily infiltrating mass. It was removed by Dr. Kannel and diagnosed as a lymphosarcoma from the gross pathological features. She was given another dose of the same Reagent, recovered, and remained well thereafter, and on last examination in April, 1946, twenty-one years after Treatment, was still found well.
This experience plus the one that follows, shows that the cause of the neoplastic effort may return in the course of years, or maybe was removed by the Treatment sufficiently to reverse the neoplastic effort, and still a seed of the cause, — an old infection in an anoxic scar, might have still escaped complete removal. Later on the cause grew to pathogenic proportions, and started trouble again. This means that the Therapy should have been repeated a year or so after, or even three years after the first neoplasm was cured, to make sure the cause was fully removed. In this case, the infected scar was not identified. If it were it could have been removed and cultured, for further information. At any rate, the dose should have been repeated before any further trouble could start. The case shows that the second Treatment was just as effective as the first, and no resistance is built up to it.
LYMPHOSARCOMA,
LYMPHOCYTE CELL TYPE
CASE No. 27
Mrs. M. S., 38 years old, came under my observation on October 27, 1944. She gave a history of a persistent crop of axillary boils that cleared up on an autogenous vaccine, but no other remedy or antibiotics helped. These appeared in April 1943, and persisted for nearly a year. During the latter part of this period the right side of her neck became stiff and painful. She could not stand a draft of air on it. Every diligent effort at treatment failed. Instead, swelling and stiffness developed and advanced deeply into the pharynx. In this bewildering condition, she stepped on a nail and sustained a severe infection of the foot. The condition in the neck became much worse then. A mass as big as an apple developed, involving the neck structures on the right side. Biopsy done October 14, 1944, and examined by several good pathologists confirmed the diagnosis of lymphocytic cell type lymphosarcoma.
Two weeks later my examination revealed a marked cachexia, and wide involvement of the palpable lymphatic system, axillary, groin and a large mass behind the umbilicus. It bulged, was hard and fixed, and could be observed on inspection.

The mass in the neck that was biopsied was 5x7 cms. in its diameters, and had infiltrated the surrounding structures even into the inside of the throat, and bulged greatly on the outside.
She received 2 cc. of the Synthetic Survival Reagent at 11 p.m. that night, and the recovery reactions started at 2 p.m. the next afternoon. Chills, fever and a general achiness as from the grippe accompanied by a relaxing of the stiffness in the neck were evident through the following three weeks. Her cachexia disappeared and her well being was being re-established. All of the neoplastic masses improved in the same way. By the end of the third week, the stiffness and swallowing difficulty was fully overcome. In three months, no more tumors could be palpated. However, her reactions were repeated at the regular periods of three months, that is the 24th, the 36th, the 72nd, the 84th, and 96th weeks and even later, and her health improved after each, in spite of the fact that her health had become much better than was normal for her, even as early as the twelfth week. Besides taking care of a large house and her family, she was able to work in a clothing shop, and carry on her social affairs. Following the absorption of the growths, there was no sudden reaction in the old site of the boils or the foot infection, as would be expected had they contributed the etiological agent. Instead, she showed a reaction in the tonsil area that presented the characteristics of a keloid. This came ten years after the cure of the lymphosarcoma. She was given a different remedy at this time, diphenoquinone, but its action was too slow. Within a year a pain in the dorsal spine developed as she had had for many years off and on since an automobile accident, some twenty years earlier. The radiographic studies by a well-respected expert gave a diagnosis of an old lesion of maybe thirty years’ standing. There was a history of suspected tuberculosis in early life, so, as a keloid is a response to tubercular toxins, and the old bone lesion that resembled a tubercular affair became evident as a reaction, our conclusion was that the lymphosarcoma was caused by the toxins of an old tuberculosis that had been suppressed.
The writer’s services were not available to her at the time, and she yielded to the persuasions of a radiologist, and took intensive X-Ray over the spine and the neck. In August 1959 she died.
In this case, a therapeutic fact was learned as in the former case of lymphosarcoma. Since lymphomas are primary protective in their intentions, one should give repeated doses every few years, a few times until there is no vestige of the exciting cause left in the system. Had this been done, this patient probably would have had no more trouble.
LYMPHOSARCOMA,
LYMPHOCYTIC CELL TYPE
CASE No. 28
Mrs. G. G., age 40, at the time of Treatment with the Survival Reagent on May 17, 1937, came for our Treatment for a rapidly developing mass on the back of her neck, toward the right side. A biopsy had been made of an enlarging gland in that location three weeks previously, when it started to grow rapidly. The microscopic diagnosis was lymphocytic cell lymphosarcoma. At the time of our examination, the scar region had become tumorous and several smaller tumors had also developed in the area. The largest was the size of the ball of one’s thumb, or an English walnut, but was deeply infiltrated. She was ill and toxic, even in spite of the cleansing regime she had followed for a week before the Treatment was given. Two cc. of the 10-(12) concentration of the Survival Reagent was injected in the upper arm. At her visit four weeks later, the whole area had normalized. No vestige of any neoplasms could be found. Her normal health had also returned and she remained well until she was killed in an automobile accident seven years later. An autopsy established that there was no trace of any neoplasm to be found, so we can assume that she was cured even without a repetition of the dose. The exciting cause was not identified in this case and no one knows if or not some interesting manifestation would have showed up later, had she not had the accident.

CANCER OF THE BREAST
The resting breast is especially prone to take on malignant change. It has plenty of FCG structures, but they are inactive and not carrying on the oxidative functions of a working tissue. The circulation has no aid as occurs in muscle containing organs where contractions pump the blood along and move the lymph, thus aiding the metabolic exchanges and extending the equilibrium point of enzymatic reactions. A blow on the breast therefore produces a dangerous injury that can interrupt the circulation and create an anoxic area much easier than in a tissue with an active circulation. Blows need not be very hard to bring about the unfavorable change, and indeed after the tumor has developed, the trauma incident to vigorous physical examination by palpation may step up the malignancy of the lesion most dangerously. For this reason America’s great diagnostician, Cullen, recommends very clever means of inspection for demonstrating the malignant infiltrations, and thus avoids the need of adverse amount of palpation. Great pressure tugging on the growth, etc., are vigorously condemned. Cullen considers even the needle biopsy dangerous. Great care, then, is used in making the examination in breast cases. The various types are so characteristic that in most cases inspection alone should settle the diagnosis, when the growth is well established.
To return the breast cancer cell to a normal functional status when it is not at work because of the normal lactogenic stimuli seems a little paradoxical. However, the restoration of the FCG does not necessarily mean it has to produce milk, but only that its impediment that blocks its dehydrogenating power is removed. When the energy producing and energy receiving Carbonyl groups are freed and able to function normally, no energy is shunted vicariously into the mitotic mechanisms to produce neoplasia.
In breast cases, the great problem is early diagnosis to give the surgeon a chance, but as the vast majority of cases are well metastasized before the lump is discovered, its early total removal by simple resection is the logical procedure to give the patient every possible chance, and then correct the Survival chemistry and teach the victim how to live.
When the breast case is under the Koch Treatment, the affected area must be kept warm. Internal cancer has a better chance to recover because of the natural normal temperature that is sustained. Breast cancer must be well covered, and must also be protected from strong sunlight, perfumes and powders women usually use. Then the examinations must be made with care, as the fine blood vessels that grow up into the coagulated and digesting mass are indeed very delicate and are easily injured. Hemorrhage at the point of vascular rupture complicates the situation, as the circulation is cut off and an excellent medium for infection is created. The continuance of the digestive process is blocked also, and one has a bad situation that may limit the recovery process at this point of injury, and indeed may prove to be the starting point for a reversal of the recovery. The patient’s responsibility for protecting the breast is a matter that must be emphasized. Of course, the physicians of experience will know what type of patient needs this advice most and will illustrate the need of care by his own manner of examination with care.
CARCINOMA SIMPLEX
CASE No. 29
Prof. R. S. L.
Miss C. F., age 50 years, Brazilian, referred by Prof. A. P. on November 17, 1941, was suffering with a painful tumor of the right breast for six months. It was considered inoperable, and 12 applications of deep X-Ray therapy were given. It continued to grow and become more painful. The nipple was already retracted, and the skin hard and infiltrated, and the whole mass was fixed to the chest wall, making it immovable to touch or by change of position, as on stooping or leaning to the side. It had become the size of a large fist. Two micrograms of Parabenzoquinone were given on November 17, 1941, intramuscularly. She recovered gradually. But six months later the dose was repeated. One year after Treatment, no tumor could be found and she was considered clinically cured.
SCIRRHUS CANCER
OF BREAST
CASE No. 30
Prof. R. S. L
Mrs. M. S. was 42 years of age and married. She found a lump in the breast in 1938, when living in Lisbon, Portugal. It was removed surgically and diagnosed cancer microscopically. Recurrence was well advanced in 1941, as a large tumor in the same location had developed as early as April, but she was not Treated until on October 14, 1941. She was given two micrograms of Benzoquinone solution intramuscularly. Examination seven months later showed that the tumor had entirely disappeared, leaving a scar isolated and no larger than a grape. Her general condition was excellent.
In the writer’s experience, the hard-calcified residues of digestion of the tumor may be removed for microscopic study. They are found to be composed of calcareous material and some dense fibrous connective tissue without epithelial structure. Right after the malignant status is corrected and calcification starts, they become subjects for removal as vascular in-growth, which may be compared with a blood clot or the casein in milk, undergoes calcification as the first step in its digestion. This is shown in Plate No. I. Then after the digestion and absorption have become complete, stones of the type described in this case may still remain. We have never seen them go malignant again, but their absorption is very slow. Whether they give any protection against cancer is not established, though we thought for a long time that they did.
METASTATIC CANCER
OF THE BREAST
CASE No. 31
Miss H. P., age 32, Canadian, was treated with the Serial System of Carbonyl groups with free radical terminals in 1927. She had been operated and the microscopic study showed a grade IV malignancy of the carcinoma simplex type. It had infiltrated the axilla and quickly showed renewed activity there and it had also metastasized to the lungs and over to the right supraclavicular space as a good sized (half egg) fixed tumor. The dyspnoea and chest signs showed heavy involvement of the mediastinum and cough was incessant.
Six months after the Treatment, there were no more symptoms or signs of the disease left. The supraclavicular space was clear, and the chest examination indicated the metastases had been absorbed. The photographs made at the time of Treatment and after recovery. In 1955 we heard from her again, that she is in perfect health and no signs of recurrence have appeared.
Miss H. P., before Treatment Miss H. P., after Treatment

FIBROMA OF UTERUS
CASE No. 32
Miss G., age 45 in December 1930, when first Treated. These are interesting cases because they are exceedingly slow to recover and often requiring a year or two to be free of the growth. The most intriguing feature in such cases is that the toxin that causes cancer is fibrogenic, that is, it stimulates fibrosis as we explain later on, and when the fibroblastic response peters out, neoplasia is due to start. The protection offered by fibrogenesis probably is due to the integration of the pathogen with the fibroblastic tissue and its neutralization in that way, so that when fibrogenesis fails, the toxin must add to some other cell structure and this seems to be the mitotic mechanism. In this connection, it is significant that neoplasms came later on in such cases. The photographs tell the story in this case. The second picture was taken after the absorption was complete. It is 30 years since her Treatment was given, and she has not developed any cancer as yet. The photographs were part of the evidence in the U. S. Federal Court.

Photograph I, before Treatment.

Photograph II, after Treatment. The recovery was complete, no vestige of the growth can be found.