Sanford
FOWLER-HAWKINS
Lung Flute
Lung Flute
Got Chemtrails ? Ashtma ? Emphysema ? Pneumonia ? Hualp with this :


http://www.lungflute.com
Medical Acoustics
640 Ellicott Street, 4th floor
Buffalo, NY 14203
Do you suffer from chronic lung congestion? Has Bronchial Hygiene Therapy (BHT) been recommended to you?
Now, thanks to the Lung Flute, you can breathe easier.
The Lung Flute is indicated for Positive Expiratory Pressure therapy, which is an important part of BHT. BHT can be used for a variety for congestive conditions such as: COPD, bronchitis, pneumonia, asthma, emphysema or other chronic respiratory ailments.
When you endure lung congestion with thick, chronic mucus that is difficult to break up, breathing can be a constant struggle. You may have to rely on medications, inhalers, oxygen therapy or even surgery to open up your airways. Everyday activities can become an effort.
The Lung Flute from Medical Acoustics can help.
The FDA-cleared Lung Flute is the only product that uses sound vibration to stimulate your body's natural mucus-clearing system – effectively thinning and dislodging mucus deep in the lungs so that it's easier to cough up. The small, reusable, plastic device is non-invasive, easy to use and drug-free – just blow into the mouthpiece and the device will do the rest.
Clinical tests have proven the Lung Flute's ability to break up mucus in the lungs, making it equally effective for both therapeutic and diagnostic use. Unlike other devices, which rely on pressure and can't reach deep lung mucus, the Lung Flute's technology is based on low-frequency acoustic waves that are produced when you blow into the flute-shaped device.
http://www.youtube.com/watch?v=CRVoP-Xptgg
Lung Flute Product DEMO - YouTube
https://en.wikipedia.org/wiki/Lung_flute
A lung flute is a medical device used to clear mucus from congested lungs with low-frequency sound waves. The device consists of a mouthpiece and a plastic reed which vibrates within a chamber to create sound waves in the chest cavity. These sound waves vibrate and break up mucus deposits in the lungs, allowing cilia to more easily move these deposits from the lungs to the throat.
Invented by acoustics engineer Sandy Hawkins, the lung flute is currently in use as a diagnostic tool in Japan, Europe, and Canada,[1] and on January 4, 2010 was granted approval by the U.S. Food and Drug Administration (FDA) for use in the United States.[2]
US6984214
/ US6702769
Device and method for inducing sputum and collecting samples
Device and method for inducing sputum and collecting samples
Inventor(s): FOWLER-HAWKINS SANFORD ELLIOT
A device for thinning lung secretions comprises a housing, a reed disposed in the housing, and an acoustical resistance. The reed produces a low-frequency audio shockwave in a range of about 12 Hz to about 30 Hz when vibrated. The acoustical resistance couples a patient lung cavity to the audio shockwave, thereby vibrating the patient's lung cavity to thin lung secretions.
BACKGROUND OF THE INVENTION
The human lungs comprise a natural means for clearing mucus. Human lungs contain tiny clearing cilia that vibrate at approximately 18 Hz. At that frequency, mucus has a significant phase change from a viscous to fluid to thinner secretions. Accordingly, the cilia operate to loosen the mucus by making it more fluid. Once the mucus is more fluid, it can be more easily expelled.
Some patients with weak lungs, disease, or other ailments have lungs that cannot create a sufficient phase change in the viscous mucus. Additionally, a doctor may need to induce a sputum sample from a patient. Accordingly, an artificial means of vibrating the lungs at approximately 18 Hz can be used to supplement the patient's natural mucus system. In some cases, an artificial means of vibrating the lungs can produce the same phase change in mucus as produced by the lungs' natural cilia.
One conventional method for artificially vibrating a patient's lungs is by using pulses of air pressure introduced through the mouth and into the lungs. However, such a method can produce dangerously high air pressures, which can damage the fragile air sacs in the lungs.
Another conventional method for artificially vibrating a patient's lungs is by using low frequency audio of approximately 18 Hz to make lung secretions thinner. Low frequency audio does not induce potentially dangerous high air pressures in the lungs that are associated with the air pulses discussed above. However, conventional methods require very high audio power to cause vibration at low frequencies. Common loudspeaker components can be used to provide a high-powered audio source for vibrating the lungs. However, the life expectancy of the high-powered audio drivers is low, and the cost of the high-powered audio drivers is high. Additionally, powered subwoofers and loudspeakers typically are not disposable or portable.
A patient's lungs and vocal cords make a particularly efficient loudspeaker in the vocal range. However, low frequencies are not efficiently produced because both the vocal cords and the lungs are too small. If the lungs could be made larger, they would support low frequency audio production, and they also would couple efficiently to a low frequency audio source.
Therefore, a need in the art exists for a system and method that can provide a low-cost, disposable, and/or portable, artificial means of vibrating a patient's lungs to cause a viscous change in mucus contained therein. A need in the art also exists for an efficient means of coupling a patient's lungs with an audio source to produce a low frequency vibration in the lungs. Additionally, there exists a need in the art for a non-powered, low-frequency audio source for artificially vibrating a patient's lungs.
SUMMARY OF THE INVENTION
The present invention can provide a device and method for artificially vibrating a patient's lungs to cause a viscosity change in mucus contained therein. The device and method can be used to clean mucus from the lungs or to induce a sputum sample for diagnostic purposes from the lungs.
The lung vibrating device and method according to the present invention can allow the lungs to produce low frequency audio that can vibrate the lungs at the desired frequency to change the viscosity of mucus. Typically, human lungs are too small to produce low-frequency audio sound. The lung vibrating device and method according to the present invention can comprise an acoustical resistance that can increase the apparent volume of the lungs, thereby allowing the lungs to produce low-frequency audio in the desired range. The acoustical resistance can allow the lungs to couple efficiently to an audio source to produce low-frequency shockwaves. The acoustical resistance can make the audio source behave as if it is operating in a much larger volume than the body cavity alone, thereby allowing low-frequency audio to be produced and considerably improving energy transfer efficiency. The present invention can generate relatively low frequencies efficiently by using an acoustical coupling technique based on Thiele-Small loudspeaker parameters.
The device according to the present invention can use the acoustical resistance to improve the transfer of audio energy to a body cavity such as the lungs. The device can produce low frequency audio and then can use the body cavity as a loudspeaker enclosure. The acoustical resistance can couple the body cavity efficiently to the low frequency sound. Additionally, the acoustical resistance can efficiently couple the sound/audio/shockwave to the body cavity to vibrate the lungs at the desired frequency. Accordingly, small and inexpensive sound sources can efficiently generate low frequency audio in body cavities.
In an exemplary aspect of the present invention, a lung vibrating device can comprise a reed disposed in a housing. A patient can blow air through the housing, which can cause the reed to vibrate and produce an audio shockwave. An acoustical resistance of the device can couple the audio shockwave produce by the reed with the lungs to produce low-frequency vibrations. Accordingly, the acoustical resistance can provide a back pressure that can transmit the low-frequency vibrations into the lungs to cause a viscosity change in mucus.
These and other aspects, objects, and features of the present invention will become apparent from the following detailed description of the exemplary embodiments, read in conjunction with, and reference to, the accompanying drawings.
BRIEF DESCRIPTION OF THE DRAWINGS
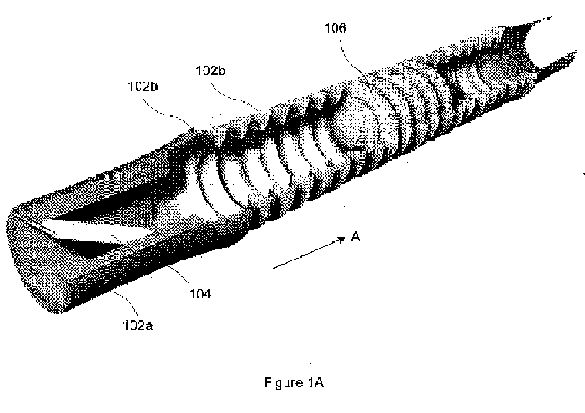
FIG. 1A illustrates a perspective, cut-away view of a lung vibrating device according to an exemplary embodiment of the present invention.
FIG. 1B illustrates a cross-sectional, side view of the exemplary lung vibrating device illustrated in FIG. 1.
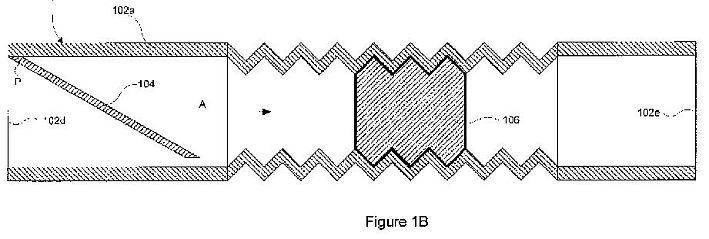
FIG. 2 is a cross section of an exemplary housing insert illustrating an exemplary embodiment of a reed disposed in a housing.
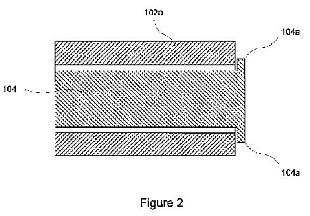
FIG. 3 is a side view illustrating a lung vibrating device according to an alternative exemplary embodiment of the present invention.
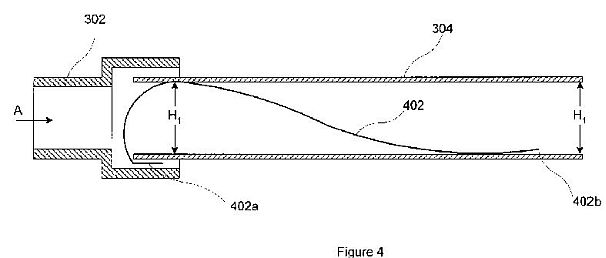
FIG. 4 is a cross-sectional view of the exemplary lung vibrating device illustrated in FIG. 3.
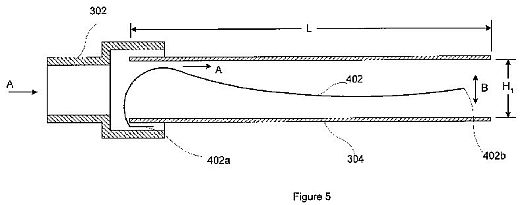
FIG. 5 is a cross-sectional view illustrating an operation of a lung vibrating device according to an exemplary embodiment of the present invention.
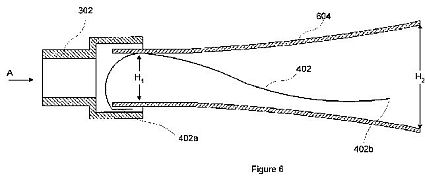
FIG. 6 illustrates a cross-sectional view of a lung vibrating device according to an alternative exemplary embodiment of the present invention.
FIG. 7 illustrates a cross-sectional view of a lung vibrating device according to another exemplary embodiment of the present invention.
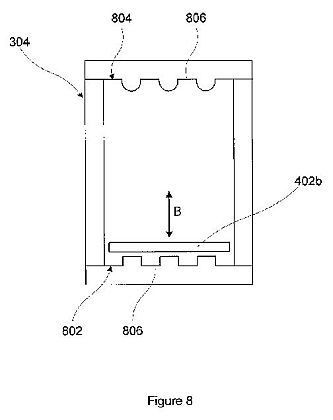
FIG. 8 illustrates an exit end view of a lung vibrating device according to an exemplary embodiment of the present invention.
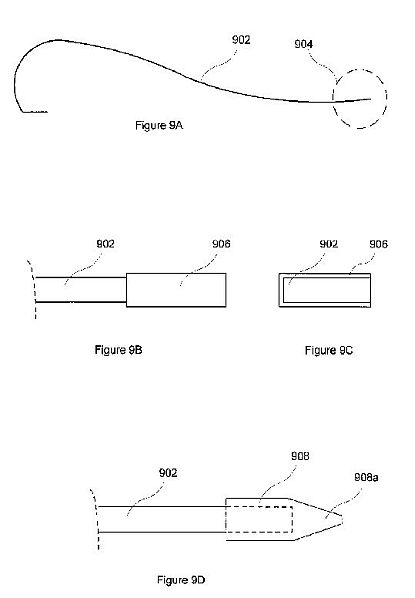
FIG. 9A illustrates a location of a reed weight according to an exemplary embodiment of the present invention.
FIG. 9B is a side view illustrating a reed weight according to an exemplary embodiment of the present invention.
FIG. 9C an end view of the reed weight illustrated in FIG. 9B.
FIG. 9D illustrates an alternative reed weight according to an exemplary embodiment of the present invention.
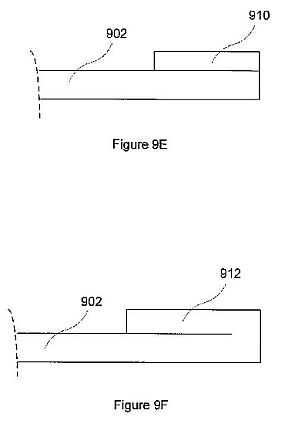
FIG. 9E illustrates a reed weight according to another alternative exemplary embodiment of the present invention.
FIG. 9F illustrates a reed weight according to another alternative exemplary embodiment of the present invention.
FIG. 10 is a cross-sectional view of a lung vibrating device according to an alternative exemplary embodiment of the present invention.
FIG. 11 is a cross-sectional view of a lung vibrating device according to another alternative exemplary embodiment of the present invention.
FIG. 12 is a block diagram illustrating an exemplary power make up device for a lung vibrating device according to an exemplary embodiment of the present invention.
FIG. 13 is a cross-sectional view of a lung vibrating device comprising sample collection carriers according to exemplary embodiments of the present invention.
FIG. 14 is a cross-sectional view of a portion of a reed and weight comprising sample collection carriers according to exemplary embodiments of the present invention.

DETAILED DESCRIPTION OF EXEMPLARY EMBODIMENTS
Exemplary embodiments of the present invention will be described below with reference to FIGS. 1-12 in which the same reference numerals represent similar elements.
FIG. 1A illustrates a perspective, cut-away view of a lung vibrating device 100 according to an exemplary embodiment of the present invention. FIG. 1B illustrates a cross-sectional, side view of the exemplary lung vibrating device 100. The device 100 comprises an unpowered, disposable audio noisemaker. As shown in FIGS. 1A and 1B, the device 100 comprises a harmonica-type, free reed 104 in a housing 102. The device 100 also comprises an acoustical resistance 106 disposed within the housing 102.
The housing 102 can comprise a standard respiratory tube or other suitable material. As shown, the reed 104 can be coupled at point P to an insert 102a disposed in the housing 102. Alternatively, the reed 104 can be provided in a separate end cap (not shown) that couples to an end of the housing 102. The reed 104 can be coupled to the housing 102, or to the housing insert 102a, by any suitable method. For example, the reed 104 can be glued or sonically welded to the housing 102 or insert 102a.
The reed 104 can be formed from any suitable material such as plastic, wood, or metal, or combinations of those materials. In one exemplary embodiment, the reed 104 can be formed of solid brass. In another exemplary embodiment, the reed 104 can be formed of Mylar. In another exemplary embodiment, the reed 104 can be a composite of several materials. For example, the reed 104 can be formed of two Mylar sheets with an inner stiffening material. The stiffening material can be any suitable material, for example, tin foil.
The efficiency of the reed 104 can be increased by providing a weight (not shown) on its free end. For a more complete discussion of weighting the free end of the reed, see the discussion below with reference to FIGS. 9A-9F. The weight can assist the reed 104 in vibrating as air flows past it. Alternatively or additionally, the efficiency of the reed 104 can be increased by providing an airfoil (not shown) on its free end. As air flows past the reed 104, the airfoil provides lift, which cause the free end of the reed 104 to rise. As the airfoil rises with the free end, the airfoil stalls, causing the reed 104 to fall.
Because the lung clearing cilia of most patients operate at approximately 18 Hz, the device 100 does not need to reproduce a wide frequency range of sound. Accordingly, in an exemplary embodiment, the device 100 can be tuned to an operating frequency of about 18 Hz, or it can be tuned to match the operating frequency of a specific patient's cilia. Matching the acoustical resistance of the device to the patient's lung cavity can make the device efficient and inexpensive. In an alternative exemplary embodiment, the device can be tuned to operate in a frequency range of about 12 Hz to about 24 Hz. In another alternative exemplary embodiment, the device can be tuned to operate in a frequency range of about 16 Hz to about 20 Hz. In other exemplary embodiments, the device can be tuned to operate at a frequency within ranges of about 12 Hz to about 30 Hz, about 20 Hz to about 30 Hz, and about 25 Hz to about 30 Hz.
Regarding the vibration frequency of the device, a reed can be tuned to vibrate at the desired frequency. Alternatively, a process called sub-harmonic doubling can be used. In that process, the reed can be tuned to vibrate at a frequency that is about double the desired frequency. However, in sub-harmonic doubling, an additional shockwave is produced at about one-half of the vibration frequency. Accordingly, the additional shockwave is produced at about the desired frequency. For example, the reed can be tuned to vibrate at about 36 Hz, thereby producing an additional shockwave at the desired frequency of about 18 Hz.
In an exemplary embodiment of the present invention, the acoustical resistance 106 can comprise a small piece of foam, a medical HEPTA filter of the desired acoustical resistance, or a cone tapering down to a smaller diameter. In another alternative exemplary embodiment, a variable acoustical resistance can be used to tune the system to a particular patient. For example, the acoustical resistance 106 can be a variably compressed piece of foam, interchangeable HEPTA filters having different resistances, or a variable shutter or valve giving an adjustable exit diameter. Alternatively, the acoustical resistance 106 can be replaced with a movable piston (not shown) disposed on the exit end of the housing 102. The movable piston can control the amount of resistance provided to air exiting the housing 102.
To use the device 100 for lung cleaning or sputum sample induction, a patient exhales through the housing 102 of the device 100 for about 3 minutes or less. As the patient exhales through the housing 102, air enters the housing in the direction A through end 102d of the housing 102 and exits the housing 102 and end 102e. The air passing by reed 104 causes the reed 104 to vibrate. The reed 104 can be tuned to vibrate at about 18 Hz (or to a frequency corresponding to the patient's cilia). The device can produce a volume of about 10 dBa to about 75 dBa. In alternative exemplary embodiments, the device can be tuned to produce a volume of about 10 dBa to about 20 dBa or about 65 dBa to about 75 dBa. The pressure resistance produced can be about 2.5 cm H2O at 100 Lpm. In terms of pressure or power, 70 dBa is about three orders of magnitude less than typical activities such as yelling or loud continuous coughing.
While the device 100 only applies about between about 75 to about 100 dBa to the airway, it can drive the thorax hard enough to feel the lungs vibrate through thick clothing. By vibrating the lungs at approximately 18 Hz, the lung secretions can become thinner, allowing the natural cleaning action of the lung's mucus pump to dispose of the secretions. After using the device 100, the secretions collect at the back of the patient's throat for approximately 3 to 12 hours. The patient then can swallow the secretions or orally expel them.
FIG. 2 is a cross section of an exemplary housing insert 102a illustrating an exemplary embodiment of the reed 104 disposed in the housing 102. To prevent the reed 104 from breaking off and being swallowed by a patient (for a patient using the proper end of the device 100 but inhaling too hard through the device), a free end 104a of the reed 104 can be made large enough that it will not fit through the end of the housing insert 102a and into the lungs.
If the device 100 is used backwards and the reed vibrates when a patient inhales, lung secretions can be driven deeper into the lungs. In an exemplary embodiment, to prevent a patient from using the device 100 backwards and vibrating the reed 104 while inhaling, one or more holes (not shown) can be provided in the housing 102 between the acoustical resistance 106 and the exit end 102e of the housing 102. The hole(s) can allow enough air to enter the housing 102 to prevent the reed 104 from vibrating. If a hole is provided in the reed end of the housing 102, it can be provided between the reed 104 and the acoustical resistance 106.
A powered system (not shown) using the non-powered disposable device 100 also can be encompassed by the present invention. An exemplary powered system can comprise an external voice coil that drives the reed 104 with a small steel element added to the tip of the reed 104. The coil can be activated alternately to vibrate the reed 104. Some potential applications such as an intensive care unit ("ICU") or neonatal lung cleaning may require an externally powered system if the patient is unable to exhale through the device. Additionally, a powered system can be useful with unconscious patients or patients with excessive lung secretions or extensive scarring. Another advantage of the powered system according to the present invention is that all parts in contact with the patients are disposable.
A powered system should not be used while inhaling, as the lung secretions can be driven deeper into the lungs. To prevent operation of the system while inhaling, the powered system can comprise a pressure sensitive flap in the housing 102 that opens on inhale, thereby reducing the acoustical coupling and the low frequency efficiency below that necessary to cause vibration of the reed 104.
The unpowered lung vibrating device 100 also can include the intake flap described above. However, the flap may not be necessary on the unpowered device, because the reed may not vibrate on inhale and the reed seal makes it difficult to inhale (if the user is blowing through the right end of the device).
FIG. 3 is a side view illustrating a lung vibrating device 300 according to an alternative exemplary embodiment of the present invention. FIG. 4 is a cross-sectional view of the exemplary lung vibrating device 300 illustrated in FIG. 3. As shown, the lung vibrating device 300 comprises a first end cap 302 coupled to a housing 304. The housing 304 can comprise a substantially uniform cross section, as indicated by the substantially equal heights H1.
The first end cap can comprise a mouth piece through which a patient blows air in the direction A into the housing 304. A reed 402 is disposed within the housing 304. The reed 402 comprises a fixed end 402a and a free end 402b. As shown in the exemplary embodiment of FIG. 4, the fixed end 402a can be compression or friction fitted between the first end cap 302 and the housing 304. In an exemplary embodiment, one of the housing 304 and the end cap 302 can comprise a positioning channel (not shown) that positions the reed 402 along a center of the housing 304. In another exemplary embodiment, one of the housing 304 and the end cap 302 can comprise ribs (not shown) that contact the fixed end 402a of the reed 402 to hold the reed 402 in place. In another exemplary embodiment, the fixed end 402a of the reed 402 can comprise a T-shape (not shown) that extends outside the end cap 302. The T-shape can maintain the reed 402 at the proper position within the housing 304 by preventing the reed 402 from slipping into the housing 304.
In alternative exemplary embodiments (not shown), the fixed end 402a of the reed 402 can be glued, sonically welded, or taped to either the end cap 302 or the housing 304. Any suitable method for coupling the reed to the device is within the scope of the present invention. In an exemplary embodiment, an entrance opening of the end cap 302 can be small enough to prevent the reed from exiting the device and being inhaled by a patient. In an alternative exemplary embodiment, the end cap 302 can comprise vanes (not shown) that reduce the open area of the end cap 302 to prevent the reed from passing therethrough.
The housing 304 can comprise a rectangular or square shape to minimize air flow around the reed 402. However, the present invention is not limited to only those shapes and encompasses other shapes. For example, the housing 204 can be circular, oval, or any other suitable shape. Those shapes may incur a slight efficiency drop, which can be compensated for by adjusting the acoustical resistance of the device.
The reed 402 can comprise any material having a suitable stiffness that will not absorb excessive energy from the vibrations. For example, the reed 402 can comprise plastic, wood, bone, metal, or combinations of those materials. In an exemplary embodiment, the reed 402 can comprise Mylar. The Mylar thickness can be in a range of about 3.75 mils to about 10 mils. In the exemplary embodiment of FIG. 4, the reed comprises Mylar having a thickness of about 5 mils and a length of about 12.25 inches.
The end cap 302 can be shaped externally to allow a patient' mouth to achieve a suitable seal around the end cap 302. For example, the end cap 302 can have a circular or oval external shape. Other external shapes that achieve a suitable seal are within the scope of the present invention. For example, the external shape can be square or rectangular.
The end cap 302 can be coupled to the housing 304 by various methods. In an exemplary embodiment, the end cap 302 can be glued or sonically welded to the housing 302. In an alternative exemplary embodiment, the end cap 302 can be compression or friction fitted onto the housing 304. In another alternative exemplary embodiment, the end cap 302 can interlock with the housing 304 through the use of a hook and latch or other suitable type of clipping device. In any case, the end cap 302 can be coupled to the housing 304 such that the air moving in direction A will not leak between the end cap 302 and the housing 304 in an amount sufficient to reduce the effectiveness of the device 300.
In an alternative embodiment (not shown), the housing 304 can be suitably shaped on its entrance end to perform the function of a mouthpiece. In that embodiment, the end cap 302 can be omitted.
FIG. 5 illustrates a cross-sectional view of the lung vibrating device 300 in operation according to an exemplary embodiment of the present invention. In operation, a patient blows air in the direction A into the first end cap 302. As the air passes in the direction A over the reed 402, the free end 402b of the reed 402 vibrates up and down, as indicated by the arrow B. The vibration produces an acoustical shockwave within the housing 304.
An acoustical resistance in the device 300 couples the patient's lungs to the acoustical shockwave to allow production of low-frequency audio shockwaves. The acoustical resistance provides a back pressure of the acoustical shockwave back through the end cap 302 and into the patient's lungs. In the exemplary embodiment illustrated in FIGS. 4 and 5, the acoustical resistance can comprise an air mass provided in the housing 304. In that exemplary embodiment, a length L and the height H1 of the housing 304 can comprise a volume sufficient to provide an air mass large enough to produce the desired acoustical resistance (and back pressure).
Additionally or alternatively, a size or compliance of the reed 402 can provide the acoustical resistance. For example, the size or compliance of the reed 402 can be increased until the amount of air required to vibrate the reed 402 is sufficient to provide the desired acoustical resistance and back pressure into the patient's lungs.
FIG. 6 illustrates a cross-sectional view of a lung vibrating device 600 according to an alternative exemplary embodiment of the present invention. As shown, the device 600 comprises the first end cap 302 and a housing 604. The reed 402 is disposed within the housing 604. The housing 604 can have a horn shape, whereby a first portion has a height H1 and a second portion has a height H2, which is larger than the height H1. Accordingly, a cross-sectional area of the first portion is less than a cross sectional area of the second portion. In operation, the free end 402b of the reed 402 vibrates up and down in the second portion of the housing 604. Accordingly, the free end 402b has additional space to vibrate up and down. Additionally, the free end 402b is less likely to contact the housing 604. The horn shape also increase the air flow through the device. The increased air flow can have several benefits. For example, the increased air flow can provide additional air that reduces fogging of the housing by drying condensation that forms on the housing. Additionally, the increased volume can increase the acoustical resistance of the device.
FIG. 7 illustrates a cross-sectional view of a lung vibrating device 700 according to another exemplary embodiment of the present invention. As shown, the device 700 comprises an end cap 702 and a housing 704. The device 700 also comprises the reed 402 disposed in the housing 704. The end cap 702 and the housing 704 can have correspondingly tapered ends 706a, 706b. The tapered ends can provide an improved compression fit between the end cap 702 and the housing 704. Additionally, the tapered ends 706a, 706b can prevent drawing and excessive amount of the fixed end 402a of the reed 402 out of the housing 704 as the end cap 702 and the housing 704 are pushed together.
FIG. 8 illustrates an exit end view of a lung vibrating device according to an exemplary embodiment of the present invention. As shown, the housing 304 can comprise four separate pieces coupled together. The pieces can be coupled together by gluing, sonic welding, taping, or other suitable means. Alternatively, the housing 304 can be molded as a single piece (not shown). The housing 304 can be formed from plastic, wood, metal, or other suitable material.
In an exemplary embodiment, inner surfaces of the housing 304 can comprise a substantially smooth surface (not shown). In the alternative exemplary embodiment illustrated in FIG. 8, a lower inner surface 802 and an upper inter surface 804 of the housing 304 can comprise one or more grooves 806. The grooves 806 reduce the surface area of the inner surfaces 802, 806 of the housing 304 that can contact the reed 402. Accordingly, any condensation that accumulates on the upper and lower inner surfaces 802, 804 of the housing 304 can collect in the grooves 806. The free end 402b of the reed 402 contacts a smaller surface area of the housing 304. Additionally, as shown by the grooves in the upper inner surface 804, the grooves can be rounded to further reduce the surface area contacting the reed 402. In an alternative exemplary embodiment (not shown), the grooves can be pointed to provide a minimum surface area that contacts the reed 402. Thus, the reduced surface area reduces adhesion of the reed 402 to condensation on the inner surfaces 802, 804 of the housing 304.
The grooves 806 also can provide other benefits. For example, the grooves 806 can provide an air path that will tend to lift the reed off the inner surfaces of the housing. Additionally, in an exemplary embodiment, a surface of the grooves can be rough (not shown). Moisture is more likely to condense on the rough surface area in the grooves 806 rather than on the smooth surface area that contacts the reed 402. Accordingly, moisture on the housing surfaces that can contact the reed 402 can be reduced.
The present invention is not limited to the shape of the groove 806 illustrated in FIG. 8. Any suitable shape that reduces the surface area of the housing 304 that contacts the reed free end 402b is within the scope of the present invention. For example, the grooves 806 can comprise a semi-circular shape, a V-shape or other suitable shape. Additionally, the grooves 806 can be provided along the entire length of the housing 304. Alternatively, the grooves 806 can be provided along only a portion of the housing 304, or along intermittent portions of the housing 304. For intermittent portions, the grooves 806 may appear more like individual squares, rectangles, or other shapes in the inner surfaces of the housing 304.
FIGS. 9A, 9B, 9C, 9D, 9E, and 9F illustrate alternative, exemplary embodiments of a weight provided on a free end 904 of a reed 902. In FIG. 9A, a reed 902 is illustrated. The reed 902 can comprise a reed as described above. A weight can be provided on the reed's free end in the location illustrated by reference numeral 904.
FIG. 9B is a side view illustrating a reed weight 906 according to an exemplary embodiment of the present invention. FIG. 9C is an end view of the reed weight 906 illustrated in FIG. 9B. As shown in FIGS. 9B and 9C, the weight 906 can comprise a weight coupled around the reed 902. In an exemplary embodiment, the weight 906 can comprise tape provided on the end of reed 902.
FIG. 9D illustrates an alternative reed weight 908 according to another exemplary embodiment of the present invention. As shown, the reed weight 908 can envelop the end of the reed 902. Additionally, the reed weight 908 can have a tip end 908a that is tapered. In an exemplary embodiment, the tip end 908a can be thinner than a thickness of the reed 902. The decreased thickness on the tip end 908a can increase the efficiency of the reed 902 to lower the frequency achievable by the reed 902. In an exemplary embodiment, the thinner tip end of reed weight 908can be provided by using a tape material having the desired thickness. Alternatively, the free end of the reed weight 908 can be tapered by grinding, or notches can be provided in the free end of the reed weight 908 to reduce the surface area of the end of the reed weight 908. In an exemplary embodiment, the reed weight can comprise tape having a thickness of about 0.5 to 1.5 mils. In one exemplary embodiment, the tape can comprise medical tape.
FIG. 9E illustrates a reed weight 910 according to another alternative exemplary embodiment of the present invention. The reed weight 910 comprises a weight disposed on an end of the reed 902. And that exemplary embodiment, the reed weight can simply increase the thickness and weight of the reed 902 at its free end. In an exemplary embodiment, the reed weight 910 can comprise a material that is the same as the reed 902. In an alternative exemplary embodiment, the reed weight 910 can comprise a material different from the material of the reed, such as tape. In another exemplary embodiment, the free end of the reed/weight combination can be tapered or notched as described above.
FIG. 9F illustrates a reed weight 912 according to another alternative exemplary embodiment of the present invention. The reed weight 912 can comprise a double portion of the reed 902. In that regard, the end of reed 902 can be doubled over onto itself to produce the reed weight 912. In an exemplary embodiment, the free end of the reed/weight combination can be tapered or notched as described above.
An area of the end of any reed/weight combination can be reduced to improve the efficiency of the reed 902. The area can be reduced by grinding to taper the end of the reed weight. Alternatively, the area can be reduced by providing grooves or holes in the free end of the weight and reed combination. The grooves or holes remove surface area of the end of the weight, thereby reducing the area.
In an exemplary embodiment, the reed weight can comprise a first material, and the reed can comprise a second material. A compliance of the first material can be in a range of about one-eighth to about one-half of a compliance of the second material. In another exemplary embodiment, the compliance of the first material can be about one-fourth of the compliance of the second material. The differing compliances can increase the efficiency of the reed.
In an exemplary embodiment, the reed can be exchangeable to allow replacement after the reed reaches the end of its useful life. Accordingly, the lung vibrating device can be reconstructed by replacing the reed.
In another exemplary embodiment the reed can comprise, either alone or with a weight, a wear indicator on its free end. The indicator can indicate to a user when the reed has reached its useful life and cannot provide the proper operating frequency. In one embodiment, the reed can comprise an inked indicator that vibrates off over the useful life of the reed.
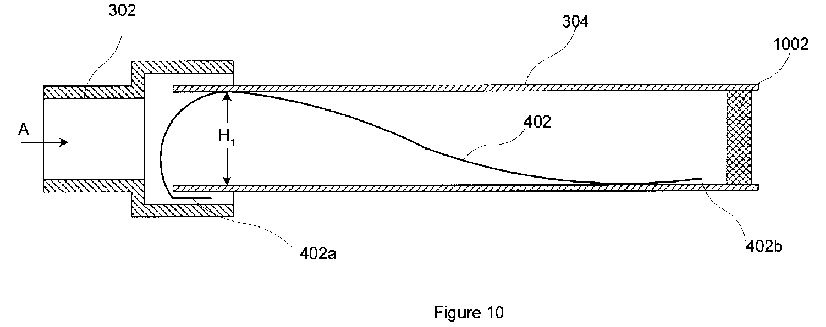
FIG. 10 is a cross-sectional view of a lung vibrating device 1000 according to another alternative exemplary embodiment of the present invention. As shown, the lung vibrating device 1000 comprises an acoustical resistance plug 1002. The acoustical resistance plug 1002 can comprise a HEPTA filter or a foam plug. Furthermore, the device 1000 can comprise additional acoustical resistances. For example, the device 1000 can comprise an acoustical resistance produced by a size of the reed 402, as described above with reference to FIG. 4. Additionally, or alternatively, the device 1000 can comprise an acoustical resistance composed of an air mass provided in the housing 304, as described above with reference to FIG. 4.
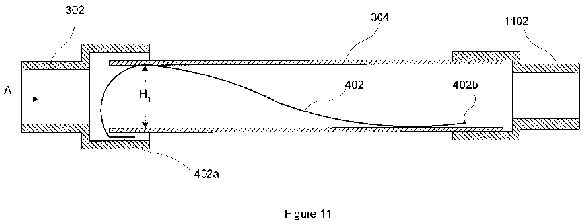
FIG. 11 is a cross-sectional view of a lung vibrating device 1100 according to another alternative exemplary embodiment of the present invention. As shown, the lung vibrating device 1100 can comprise a second end cap 1102 provided on the housing 304. The second end cap 1102 can function as an acoustical resistance by restricting the air flow from the housing 304. Additionally, the second end cap 1102 can provide a means to connect the device 1100 to a respirator. In an alternative exemplary embodiment, the second end cap 1102 can provide a means to connect the device 1100 to a respirator without serving as an acoustical resistance. When connected to a respirator, the respirator can draw air through the housing 304 to drive the reed 402 to produce the acoustical shockwave in the patient's lungs.
FIG. 12 is a block diagram illustrating an exemplary power make up device 1200 for a lung vibrating device according to an exemplary embodiment of the present invention. As shown, a fan 1202 can push air through a duct 1204 in the direction of the arrows A. The duct 1204 can comprise an aperture 1006. An exit opening of a lung vibrating device 1208 can be provided in proximity to the aperture 1206. The air moving in the direction A within the duct 1204 can draw air in the direction B through the lung vibrating device 1208. Accordingly, the power make up device 1200 can produce at least a partial vacuum in the lung vibrating device 1208 by drawing air from the lung vibrating device 1208 in the direction of the arrow B. In an exemplary embodiment, the device 1200 can produce about 1.5 inches of negative water pressure in the lung vibrating device 1208.
As evident to those skilled in the art, the lung vibrating device according to the present invention can incorporate many features not illustrated in the attached figures. For example, exemplary embodiments can comprise a space-saving design, incorporating a foldable, hinged, or telescoping housing. Another embodiment encompasses a device formed from a thin material that can be crumpled and disposed.
The lung vibrating device can be used to perform many functions. For example, the device can be used to induce sputum to clear the lungs or to provide a diagnostic sample, improve muscillary clearance post operatively, prevent lung collapse (atelectasis), improve oxygenation, improve lung capacity or lung clearance in athletes prior to performance, or treat smoke inhalation.
The efficient coupling of an audio source and a body cavity to produce low-frequency sound can be used for other applications. The acoustical resistance can be adjusted to provide the proper frequency based on the particular application. Additionally, the reed can be tuned by changing its size, shape, or material to provide the proper frequency. For example, other applications can include the following:
Coronary Plaque: One application can be erosion of coronary arterial plaque by vibration. An adaptation of the powered system may erode coronary arterial plaque by internal thoracic vibration, which would be a useful clinical application.
Sinus and Ear: Several variations of the powered and non-powered lung cleaning systems can be used for sinus drainage and middle ear clearing. Operation requires a simple frequency adjustment of the lung cleaning system by an adjustment of the acoustical resistance. For uses such as sinus drainage and middle ear clearing, the systems can operate in a range between about 15 Hz and about 60 Hz with an output of from about 75 dBa to about 100 dBa. The systems also can operate between about 40 Hz and about 60 Hz, and at about 44 Hz.
Diagnostics: A lung vibrating device according to the present invention can provide the basis of a sophisticated diagnostic tool for lung diseases such as pneumonia, COPD, asthma, and lung cancer. The diagnostic system can monitor the voltage to current phase of the loudspeaker motor and then derive the dynamic compliance of the lungs at different frequencies and different pressures and vacuums. Lung compliance varies with different secretion loads and also shows changes in elasticity caused by long term lung tissue deterioration. Accordingly, the results can be correlated with existing conditions. Early asymptomatic results also can be correlated with later disease conditions.
Intestines/Colon: Another application is to efficiently couple a patient's colon to an audio source to clean the patient's intestines or colon. That application can remove intestinal blockages, which can prevent such blockages from causing a dangerous infection.
Lung Sample Collection and Diagnostics: In another exemplary embodiment, the low-frequency sound lung vibrating device of the present invention can be used to collect lung or other body cavity samples through absorption, precipitation, or condensation. Additionally, an indicator drug can be placed in the lung vibrating device to detect the presence of specific biological materials when contacted by a collected sample.
In an exemplary embodiment, a lung vibrating device can comprise a sample collection carrier that collects a diagnostic sample exhaled from the patient's lungs. The sample collection carrier can comprise any suitable carrier for collecting a liquid, solid, or air sample from the material expelled or exhaled from the patient's lungs through the lung vibrating device. As the patient exhales through the housing of the lung vibrating device, portions of the exhaled air condense within the housing. The sample collection carrier can collect the condensate for use as a diagnostic sample. Additionally, the sample collection carrier can collect moisture within the air expelled from the patient's lungs, and the sample collection carrier can collect a solid material the contacts the carrier when expelled from the patient's lungs. Then, the sample collection carrier can be removed from the lung vibrating device to test the collected sample. Alternatively, the lung vibrating device and/or the sample collection carrier can be rinsed with distilled water. The rinse water will wash the collected sample from the sample collection carrier. Then, the rinse water can be collected and tested.
Additionally, the sample collection carrier can comprise an indicator drug or liquid that tests for the presence of specific biological materials in the collected sample. For example, the indicator drug or liquid can react chemically with specific biological materials of the collected sample, thereby changing color or texture to indicate the presence of the biological material in the collected sample.
Using a sample collection carrier with the lung vibrating device of the present invention can obtain improved lung samples. The lung vibrating device can loosen the lung secretions, thereby allowing the patient to exhale air and secreted material from deep within the lung cavity.
Exemplary sample collection carriers will be described with reference to FIGS. 13 and 14. FIG. 13 is a cross-sectional view of a lung vibrating device 1300 comprising sample collection carriers according to exemplary embodiments of the present invention. FIG. 14 is a cross-sectional view of a portion of a reed 1402 and weight 1404 comprising sample collection carriers according to exemplary embodiments of the present invention.
In an exemplary embodiment the sample collection carrier can comprise an absorbent reed 1302. The absorbent reed 1302 can comprise a material such as paper, cloth, fiber, foam, or other absorbent material that absorbs samples as the patient exhales through the housing 704 of the lung vibrating device 1300. If desired, a spine (not shown) of suitable stiffness can be coupled to the absorbent reed 1302 to produce a reed that will vibrate at the desired frequency.
In another exemplary embodiment, the sample collection carrier can comprise an absorbent weight 1304 on the end of the reed 1302. The absorbent weight 1304 can comprise a material such as paper, cloth, fiber, foam, or other absorbent material that absorbs samples as the patient exhales through the housing 704 of the lung vibrating device 1300.
In another exemplary embodiment, the sample collection carrier can comprise perforations 1408 or indentations 1406 in the reed 1402 or in the weight 1404 on the end of the reed 1402. The perforations 1408 or indentations 1406 collect the diagnostic sample by collecting condensation as the patient exhales through the housing of the lung vibrating device.
In another exemplary embodiment, the sample collection carrier can comprise absorbent strips 1305 coupled to an inside wall of the housing 704 of the lung vibrating device 1300. Alternatively, the absorbent strips can be coupled to the reed. The absorbent sirips 1305 can comprise a material such as paper, cloth, fiber, foam, or other absorbent material that absorbs samples as the patient exhales through the housing 704 of the lung vibrating device 1300. The absorbent strips 1305 can be coupled to the housing 704 by adhesive, tape, or other suitable meam. For example, the bousing 704 can comprise a pocket, frame, or other suitable holder (not shown) into which the absorbent ships 1305 can be inserted and removed.
In another exemplary embodiment, the sample collection carrier can comprise indentions 1306 on an inside of the housing 704. The indentations 1306 collect the diagnostic sample by collecting condensation as the patient exhales through the housing 704 of the lung vibrating device 1300. In another exemplary embodiment, the sample collection carrier can comprise indentation strips 1308 of rigid or semi-rigid material having indentations, which can be placed inside the housing 704 of the lung vibrating device 1300. The indentation strips 1308 can be placed loosely in the housing 704. Alternatively, the indentation strips can be coupled to the housing 704 by adhesive, tape, or other suitable means. For example, the housing 704 can comprise a pocket, frame, or other suitable holder (not shown) into which the indentation strips 1308 can be inserted and removed.
In another exemplary embodiment, the sample collection carrier can comprise protrusions 1310 inside the housing 704 of the lung vibrating device 1300. The protrusions 1310 can increase the surface area of the housing 704, thereby providing more area onto which condensate can collect. The sample can be collected by rinsing the housing 704 with distilled water and collecting the rinse water.
In another exemplary embodiment, the sample collection carrier can comprise a cup-shaped protrusion 1312, with the opening in the cup facing the mouthpiece of the lung vibrating device 1300. The cup-shaped protrusion 1312 collects condensate and prevents the condensate from exiting the housing 704's exit end.
In another exemplary embodiment, the sample collection carrier can comprise an absorbent acoustical resistance disposed in the housing. For example, the acoustical resistance can comprise an absorbent foam acoustic compliance plug. The plug absorbs the condensate as the exhaled air passes through it.