“First my trouble started in my finger tips with throbbing. It
seemed as if the blood circulation was half stopped. My hands
began to swell and I could not wear my rings any more. I had
terrific pains and then I began having trouble with my legs. I
began to have contraction of the muscles, my toes would draw up
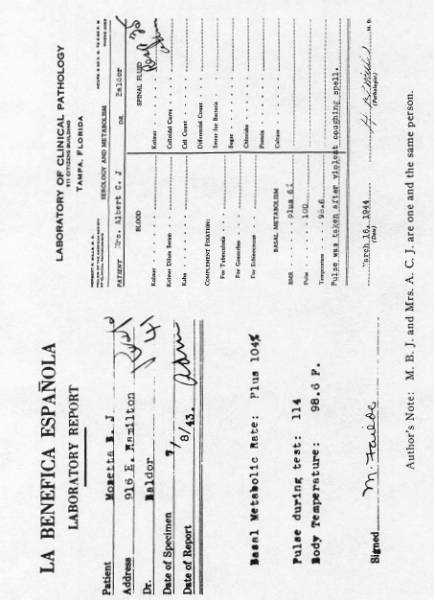
into knots. I went to Dr. Baldor about it. He gave me one thing
after another, but I did not improve any. He sent me to the
clinic for the metabolism test, and after that he started a
different treatment. It was some drops. All the time I was
taking on like crazy. I could not sleep at night. My husband had
to lift me up in bed. My hands and legs got steadily worse.
Finally I got so bad, my husband had to pick me up and put me in
the car. I could not get in. My legs would just turn to water.
Dr. Baldor gave me the Koch Treatment. About two or three weeks
later, I felt like a new woman. My strength came back, my legs
and hands cleared up, and I can use them again. I now have a job
demonstrating. I carry a suit case weighing fifty pounds in and
out of homes.”
The Basal Metabolism
Rate was taken three months after the Treatment, and found to
be perfectly normal, namely plus 6, and physical examination
showed her normal in all other respects, no sweating, no
jerking, no tremor, no muscle twitches. The exophthalmus had
completely disappeared, and so had the thyroid tumors. The
thyroid gland was normal on palpation, inspection and
function. The pulse was normal 80 to 90, and so was the blood
pressure, 140/80. She was strong, slept well, and without any
trace of the former disease.
An analysis and
interpretation of this case notes two toxic states — one that
is the result of the forced secretion of the thyroid cells,
the thyrotoxicosis that nearly killed the patient. The
other is the toxin that blocked the regulated energy
production and the regulated energy acceptance and utilization
in both the thyroid cells and the tissues in general. This
is the pathogen toxin, which the Postulate identifies as an
amine of higher O/R potential than the functional Carbonyl
(FCG) group of the tissue cells that could dehydrogenate and
thus burn out of the way. The pathogen toxin therefore
had the upper hand and as it was being increased in amount,
its effects were also increasing as the block to energy
production and energy acceptance by the tissue functional
Carbonyl groups. These normally initiated oxidations that
produce energy efficiently, and received energy in a regulated
way to perform work.
As a result the
Krebs Cycle energy production took over, and had already
largely replaced the high efficiency oxidations of the FCG’s,
when the patient came under observation of Dr. Baldor. If the
toxic amine pathogen had been subject to dehydrogenation at
the hands of the FCG, like the usual run of pathogens and fuel
substrates, it would have been burned out of the way and would
not have condensed with the FCG of either the high efficiency
energy producing system, or the FCG of the energy accepting
system of the cell, and blocked their functions.
It was evident
clinically that energy was not reaching the working
mechanisms. This was seen in the steadily increasing weakness
of the skeletal and heart muscles and nervous system. It was
also clinically evident that energy production was going on at
the highest rate shown by the BMR of 104%. It was also seen
that the thyroid gland was forced to the limit in producing
its secretion to push cell activity to evolve more energy. But
no matter how much was produced even to the exhaustion of the
patient, none was used by the energy-starved cells. The
patient lost weight rapidly and to the extreme to supply
material for energy production, but it could not get into the
working mechanism via the blocked Carbonyl groups of the
energy accepting system of the Postulate. The basic pathology
then was the block to energy acceptance by vital working
units. Since one toxin, an amine of high activation
was the pathogen, it is also evident that the FCG’s of energy
production and energy acceptance are similar atomic groups and
since these are dehydrogenators, the Postulate identifies them
as highly activated Carbonyl groups. This conclusion is
supported by the type of response to oxidation the integrated
toxin gives, after it is condensed with the tissue cell FCG’s.
That is, the type of cleavage observed is that of an
azomethine double bond when its alpha positioned hydrogen atom
actually invites dehydrogenation and is removed so a free
radical can be formed and add molecular oxygen to become a
peroxide free radical which, accomplishes the oxidative
separation with restoration of the functional Carbonyl groups
of the tissue cell and the toxic amine group is burned away.
The facts of the case history support this explanation. (See
Appendix).
It is seen here that
the pathologic state actually invites correction, and any
clinician would suggest correctly how it could be done. He
would say, since the FCG cannot dehydrogenate the toxin
and start its combustion, because its O/R potential is too
low, then the thing to do is to offer a Carbonyl group of
higher activation with a potential equal to the job. This
is what was done in this case. A molecule of correct steric
advantage carrying a Carbonyl group of high O/R potential was
used. The results were the rapid reversal of the pathogenesis.
As soon as the integrated toxin was burned out of the way,
energy could enter the cell working units, and the urgent call
for more energy stopped. The thyroid was not called upon to
whip up the tissues to do more oxidizing, and the nodules it
had developed to aid its work subsided and disappeared. The
BMR dropped to a normal of plus 6%, and all of the symptoms of
the thyrotoxicosis, and of the basic pathogen disappeared. The
woman was normal in 3 months after one dose of a highly
activated Carbonyl compound.
This case proved
a few things in the Koch Postulate, and it also shows
that the thyroid secretion takes no part in the oxidation
process, any more than the poisonous nitrophenol series, that
some have classified as accelerators of the oxidations. As we
pointed out here, the thyroid function is to whip up the cells
to put their oxidation apparatus to work to supply the energy
needed for the occasion. It itself does not enter the
oxidation process. Nitrophenol blocks various esterifications
with phosphoric acid which normally form high energy carrying
phosphate bonds. Thus it starves the cells of energy and the
tissues are whipped up to produce more energy for survival,
just as in the case at hand. Nitrophenol thus works as an
“uncoupler” and is so classified. It prevents the energy
accepting mechanisms from receiving the energy. In the case at
hand, the energy came to the doors of the energy accepting
mechanism, the FCG of energy acceptance, but the door was
closed, — blocked by the condensation with the amine compound.
Thus the Carbonyl
group of energy acceptance was already occupied and could not
condense with the amine of the ATP that carried the energy
that would be liberated by ATP-ase with the help of calcium. Our
Postulate goes on to explain that with the liberation of
energy by the hydrolysis of the ATP to ADP, the phosphoric
acid set free can split the azomethine bond setting the ADP
free to again do another cycle of energy transport with the
acid.
One sees that there
is no similarity in the actions of the thyroid secretion, the
nitrophenols and the highly activated dehydrogenator Carbonyl
compound (SSR) used to oxidize the pathogen out of the way.
The SSR actually took the leading part in the oxidation
mechanism and did the work the normal oxidation initiator
would have done, if it had an adequate O/R potential. It is
not possible to compare a reagent that prevents energy storage
for use in work, with an agent that produces energy for use in
work, and besides, actually starts the oxidation process in
the cell by burning away the pathogen that was blocking energy
production.
Further, the
nitrophenols are pathogens whose action can wear out, if not
forced too long. But if they are forced too long, they are
subject to reduction to aminophenols, which would then act
much like the pathogen in this case, and block the initiation
of the oxidation progression, and bring about a dangerous
situation much like in the case at hand. The nitrophenols
proved to be pathogens in the attempt to beautify obese
patients. The reduction in weight took place but, in too many,
the destructive action continued because of the situation that
existed in the case we are discussing, and these victims went
on to their deaths. They need their FCG’s freed from the
obstructive amine as was accomplished in this case. However,
the experts are still at sea with regard to the true action
that caused the fatalities.
The block in the use
of the energy of oxidation by dinitrophenol is seen also in
its inhibition of mitosis in Sea Urchin eggs reported by
Clowos (1951 Ann. N. Y. Acad. of Science). Even though
the dinitrophenol in doses of .01 mm concentration caused a
fourfold increase in the consumption of oxygen, the mitosis
and phosphorylation was cut in half, and further increase in
the concentration of the poison completely blocked mitosis and
phosphorylation. So whether the oxidation process is blocked
in producing energy, in transferring and carrying energy in
phosphate bonds, or in receiving this energy, the reactive
response is to produce more energy to make up for the energy
starvation, in the tissues whose working mechanisms do not
receive the energy. Thus an analysis of effects of toxic
amines and nitrophenols shows they do not give impetus to the
oxidation mechanism, but block its ultimate purpose—the supply
of energy to the vital mechanisms of the tissues. Here we find
in 1951, a nice confirmation of our Postulate measured with
microscopic accuracy.
The thyroid
secretion is a hormone whose intimate action is still unknown.
However, it does not take any part in the oxidation process
itself. Comparing its action with that of the SSR, one sees
that the latter took the leading part in the oxidation
mechanism. Further the action of nitrophenol and of thyroid
extract are of different orders and challenge comparison. The
former always has a toxic action, the latter is physiological,
but the action of both, as explained before, is very different
from that of the SSR. The high BMR in the case at hand, has a
pathologic cause depending on the pathogen that blocked energy
acceptance by the cell’s working mechanism.
The statement of
some biochemists that the oxidation process has no
immunological significance is based on the fact that the
Krebs Cycle has none. We gave the reasons before. The
O/R potentials of the participants are too low. Then these
biochemists also hold that the Krebs Cycle is the only
mechanism concerned in the tissue oxidations, and is all
sufficient. They do not consider that the Krebs Cycle is a
hang-over from the process used by primitive forms as
bacteria and though it is retained by the higher forms as
animals and man, it is only used by such as an alternative
pathway, when the High Efficiency System already explained
is inactivated for a time. That it offers no protection is
seen. Moreover, it gives no clues to the explanation of
the Pasteur Effect. The early Chapters of “The Survival
Factor in Neoplastic and Viral Diseases” show how both
depend on the action of the FCG. While the Carbonyl group that
initiates the oxidations of the High Efficiency Smokeless
System, lacks the high O/R potential Carbonyl dehydrogenator,
that some pathogens require for their destruction, yet its
range of O/R potentials is twice as high (0.7 v) as that of
the Krebs Cycle participants (0.3 v). So the opportunity to
give protection by the High Efficiency System is considerable,
— enough to maintain good health under the usual
circumstances. The use of a Super-high Carbonyl dehydrogenator
of correct steric advantage is proven, in this case, to offer
protection by way of an oxidation process that imitates that
Postulated for the High Efficiency System, and a close
analysis of this case is all that is needed to prove the
existence of the High Efficiency System.
However, two more
cases will be submitted to show that the toxic basis for
malfunction can be removed, and the pathology corrected by the
processes of adequate dehydrogenating efficiency, started by
the Super-high dehydrogenator, and continued by the natural
dehydrogenator (FCG) system.
POST-PNEUMONIA
NEPHRITIS
CASE
No. 2
Dr. Evans
Tom E. 4 years old,
was recovering from bilateral bronchopneumonia, when suddenly
he took a convulsion of considerable severity. Oedema rapidly
developed with blurred vision, headache, dizziness, delirium,
etc. The urine secretion diminished as the oedema rapidly
increased. The blood pressure was found to be 146/68, and the
blood non-protein nitrogen 74.6 mgms %. Twelve hours later the
pressure rose to 160/100, and two days later it was 180/130
showing a rapid development of the pressor substance that
blocked the kidney elimination. The oedema had developed by
then to the point where the contours of the chin and neck were
obliterated, and very little urine was passed. Then the second
convulsion took place. It was severe and the boy passed into
coma. It was in this condition that he received the Synthetic
Survival Reagent. A few hours later, the mental symptoms had
improved, he came out of the coma; soon the headache, blurred
vision, delirium, etc., gave way to rational mental comfort,
the blood pressure steadily dropped and the urine increased as
the oedema disappeared. The blood pressure was found normal in
a few days with a normal non-protein blood nitrogen of 25
mgms.%. The correction was completed by rescuing the FCG so it
would go back to work again. The pressor substance is well
known now to be a toxic amine, so our Thesis is supported
nicely by this case also.
ECLAMPSIA
CASE No. 3
Dr. Baldor
Mrs. D. was married
seven years and could never carry a baby to term. Abortion was
required before the end of the second month of pregnancy each
time, and the period was shorter each time. This was the 4th
pregnancy, and they all followed the same course and symptoms
but with increasing severity. In each instance she vomited
profusely, with much salivation constantly; the urine was
progressively decreased until only blood came, just as in the
last hours of the parathyroidectomy intoxication. Convulsions
followed by coma called for immediate abortion, if life was to
be saved. This time, however, Dr. Baldor tried the Synthetic
Survival Reagent as her big ambition in life was to have a
baby. Twenty hours after the injection was given, vomiting had
decreased from 20 times a day to twice per day. The urine
increased and, in 72 hours, she was passing half a liter a
day. This urine still carried blood and albumen. In four days,
she passed a full quart of urine per day. The vomiting
disappeared entirely within two weeks, but the salivation had
continued and, during the third week, vomiting started again.
She was given another dose of the Survival Reagent, and all
cleared up quickly thereafter. No more symptoms of eclampsia
returned. She carried her baby comfortably into the seventh
month, when she had an automobile accident, and spontaneous
abortion threatened, so she was delivered of a 5½ pound baby
that thrived well. She had no return of eclampsia symptoms and
gained full health quickly.
Here we see again
that the toxin that blocked the oxidations of function and the
regulated energy acceptance by the working mechanisms, could
be removed by an atomic group similar in kind but of higher
O/R potential. The allergic uncontrolled spasms of the small
blood vessels, and the anoxia caused by colloidal gellation,
had to yield to restored efficient FCG function. The basic
pathology was met and corrected, at its very inception. Still,
some of America’s greatest biochemists and clinical experts
claim that “the oxidation mechanism has no significant
action or position in the maintenance of health or in the
combat against disease.” They are limited, of course, by the
performances of the Krebs Cycle, which to them is the whole
oxidation mechanism. But, if one were to accept such a
dictum, one would have to add, “it is impossible to die of
asphyxia.” The predicament is rather contrary to
progress.
TOXIC GOITRE AND
CANCER OF THE STOMACH
CASE No. 4
To show that one
toxic agent (removable by one corrective attack) can cause a
toxic hyper-function as in Case I, and also cause a
very high-grade malignant neoplasm of the stomach in the same
person and at the same time, the case of Mrs. W. is offered.
At the time this
patient was treated, the Geiger Counter had not yet been
invented, so it was impossible to estimate the earth’s
irradiations in her environment. However, it is noted that she
lived in what is known as the goitre belt, a region of iodine
deficiency and also of high cancer mortality rate. Her
daughter had been treated for a rapidly developing brain
tumor. Many other patients came from this region for
Treatment. However, one thing this study lacks is a systematic
correlation of the terrestrial radiations with cancer
incidence and also the number of conditions allied to cancer
to be met; and most of all, how the terrestrial rays affect
the recovery rates both of the neoplasms and of the allied
diseases.
There was no history
of cancer in the ancestry, but her husband died of cancer 8
years previously, and her daughter, with a very malignant
tumor, was only 28 years of age as compared with the patient’s
age of 58 years, at her first visit. One recognizes here the
vigor of the carcinogenic flux of this region. Both the mother
and daughter made typical recoveries under the Treatment.
There was nothing in the geophysical environment that
interfered with the cyclic reactions and the steady progress
of the recovery process. One feature to be noted is that as
cancer is associated with aging processes, this patient, at
only 58 years of age, looked like a person twenty to thirty
years older. The skin and tissues in general were senile,
though the hair was not grey. During the recovery process the
senility changes disappeared. The main features were as
follows:
The disease started
two and one-half years previously as a steadily increasing
nervousness, progressive cardiac weakness, tachycardia,
increasing ease of perspiration, loose bowels, and tremor of
characteristic hyperthyroid type. Radiographs showed
considerable enlargement of the heart and mediastinal shadows
early in 1927. There was dyspnoea on slight exertion or lying
down. Exophthalmus developed rapidly, the skin was bronzed,
and gastric distress and inefficiency set in. The feet and
ankles swelled considerably, yet she lost weight, falling from
150 pounds to 108 pounds in less than nine months.
The physical
examination revealed the exophthalmus as shown in the
photograph before Treatment. There was also a greatly enlarged
lymph gland (walnut size) in the left supraclavicular space;
the veins of the head and neck engorged with blood when she
laid down, and percussion showed a marked increase in the
mediastinal dullness.
Examination showed
the epigastrium and the whole area below the costal border
down to two centimeters below the umbilicus on the right side
to be occupied by a huge, bulging, solid, fixed, irregular
tumor. The stools showed decomposed and occult blood. There
was vomiting and great weakness and considerable pain
throughout the abdomen. Thus the stomach, the liver, and
probably the suprarenal glands were involved by the neoplasm.
At the time of this examination she was very weak.
Mrs. W. before
Treatment showing the exophthalmus from toxic goitre excited
by the carcinogenic toxin. (Left photo)
Mrs. W. after
Treatment and recovery from cancer of the stomach, and toxic
goitre as secured from one chemical reagent. The exophthalmus
is gone for good. (Right photo)

One dose of two cc. of a 10-(12) solution of the (SSR) serial
Carbonyl system was used on September 28, 1929. The recovery
process exhibited the usual cyclic three-week reactions, with
chills, fever, and general aching, and with improvement
following each reaction until the recovery became complete. At
last report, ten years later, she was in good health. We lost
track of her thereafter.
Regular FCG
function, both for producing and using ATP energy, was blocked
and this showed for the thyroid cells, the stomach growth
mitotic mechanisms and the general tissue oxidations as
demonstrated by the senility changes. Still the Krebs Cycle
oxidations went on, and fermentation supported the neoplastic
cells. Had we supplied a Carbonyl group of FCG oxidation
potential, we probably would have gained nothing. However, a
Carbonyl group of boosted O/R potential cleared the
inactivator of FCG functions away so normal FCG metabolism (in
contrast with the Krebs metabolism) was restored, senility,
toxic goitre, and cancer all faded away permanently.
TOXIC GOITRE AND
ETIOLOGICAL TOXIC FOCI
CASE No. 5
Dr. Jayme Treiger
In this case the
pretreatment control or observation period lasted from
September 12, 1953 until March 13, 1958. The development of
the etiological factors with the progress of the disease
itself was well noted.
Mrs. D. S., F. 27
years old, married, a thin brunette woman, very nervous,
complained of dyspnoea, cold sweating, pharyngeal spasm
(sensation of an egg in her throat), able to bear heavy duties
but not simple ones, urine sometimes fetid and strongly
colored, acne, leukorrhea, sometimes bloody, and painful
nodules in the right breast. These breast symptoms arrived
after a second electro-coagulation of an ulcer on the cervix
uteri, produced after the second childbirth. These nodules
were helped by hormone treatment for a while but had returned,
with further toxic symptoms as a tachycardia of 106 per
minute, and slight thyroid enlargement, that started nine
years previously. She had pertussis, measles and vericella
during childhood.
During and since
childhood, she had periodic crises of angina with high
temperature and pus from the tonsils. Homeopathic treatment
helped the tachycardia and the throat spasms and made her feel
much better, but the basic pathology was not retarded, and she
went to a gland specialist who treated her from November 1954
to January 1956. From him she received Dexamyl, Somniphene,
Prometron, Ovocycline, Diiodotyrosine, Apliotil, Thiouracil,
and Nodular on different occasions. She did not improve on
this series of modified benzene rings, though enough were
tried. This shows that the therapeutic conception was not
based on physiological considerations, but was the fruit of
modern pharmacology.
Feeling worse, she
returned to Petropolis. The B.M.R. by Dr. T. showed a plus 45
and Cholesterol of 122 mgms. % on 3/12/58. She was now
exhausted, extraordinarily excited, always tired, difficult to
sleep, with frequent nightmares, pulse 106 per minute, and her
blood pressure in a low range. She was given 2 millimicrograms
of the SSR intramuscularly on March 13, 1958, and the
reactions that followed are indicative of the sources of her
toxins.
Reactions:
Tonsillitis that was suppressed from activity while under the
phenolic treatments mentioned above, started to be active with
high fever, pus discharge and pain in violent periodic crises.
The bloody drainage from the cervix uteri that was suppressed
by the cautery started up again. However, one week after the
Treatment in spite of the strong angina crises, she was
feeling very well, as if with renewed vitality. A few weeks
later she reported again. The pulse was normal, 82 per minute,
the blood pressure normal 120/90, and as her good health was
being restored, old symptoms of years of little difficulties
returned briefly and disappeared. She felt good enough to not
need a doctor. The throat had normalized and the cervix uteri
had healed, and she did not return for more observation. She
had received two injections of the SSR, the second one a year
after the first, for while the cervix showed no abnormality on
examination, there were symptoms suggesting reaction in the
deep scars within. The BMR in February, 1960 showed 6% over
normal, the breasts, tonsils, uterus, nerve responses were
normal, temperature 36.7°C, pulse 60, the B.P. 110/70, and she
enjoying the best health she had ever experienced.
In this case the
etiological lesions that brewed the toxins that attacked the
breast tissues and the thyroid gland were respectively the
cervix infection and the tonsil infection. The cautery sealed
up the drainage facilities, and made the scar tissue that was
infected more anoxic. The reactivity of the
reticuloendothelial cells of the tonsils to their contained
infections was suppressed by the phenolic derivatives, so the
thyroid was poisoned all the more. Further, the poisons from
the cervix and those from the tonsils while showing some
specificity to the thyroid and breast tissues were also
general poisons and affected all of the tissues making her
nervous and weak aside from a special thyroxin effect. Here
the relation of the reactions (following the Treatment with
the SSR Reagent, which were severe) to her improvement in
tissue function showed that these reactions were not of a
vaccination nature, but were actual reticuloendothelial
battles against the disease agents going on in conjunction
with the chain oxidation of these agents. Then, too, as the
various FCG units were liberated from combined toxins and went
back to work, she started to feel normal and her various
functions behaved normally again. It is to be recalled that
after the SSR was given the tonsils became acutely inflamed,
and the cervix lesion broke loose with a strong inflammatory
process. Thereby both lesions were cleared of their imprisoned
germs and fibrosis integrated pathogens, and as the induced
oxidations burned the pathogens away, the fibrosis disappeared
also. The anoxic centers were wiped out, so the disease was
cured right at its very inception. She has no more sore
throats nor cervix troubles, and no more secondary effects, as
thyroid enlargement or abnormal function. The breasts have no
more nodules either. Her general health is normal. Her nervous
system is steady. She sleeps normally and does not sweat as
she formerly did. In other words, the pathology was fully
reversed and discarded. This same course will be seen in the
other cases reported here, and in all others when one takes
the trouble to thoroughly check the recovery course.